

Diazoxide Choline Extended-Release Tablet in People With Prader-Willi Syndrome: A Double-Blind, Placebo-Controlled Trial
- PMID: 36639249
- PMCID: PMC10271219
- DOI: 10.1210/clinem/dgad014
Diazoxide Choline Extended-Release Tablet in People With Prader-Willi Syndrome: A Double-Blind, Placebo-Controlled Trial
Abstract
Context: Prader-Willi syndrome (PWS) is a rare neurobehavioral-metabolic disease caused by the lack of paternally expressed genes in the chromosome 15q11-q13 region, characterized by hypotonia, neurocognitive problems, behavioral difficulties, endocrinopathies, and hyperphagia resulting in severe obesity if not controlled.
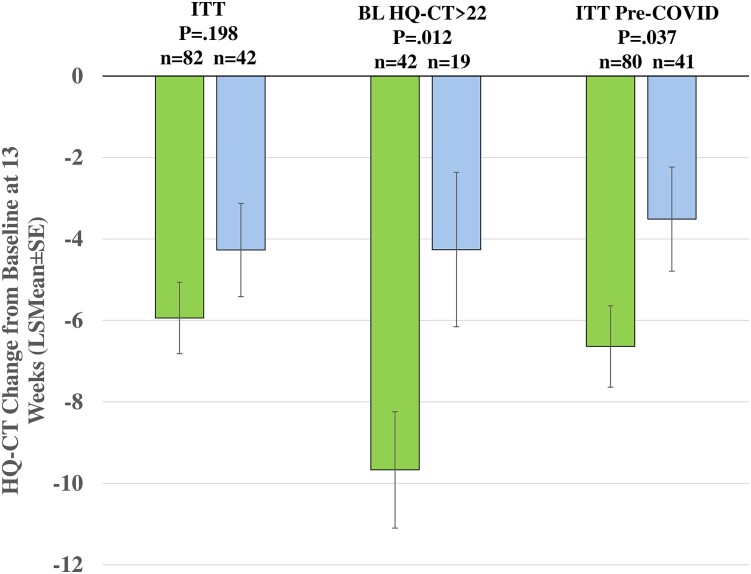
Objective: The primary end point was change from baseline in hyperphagia using the Hyperphagia Questionnaire for Clinical Trials (HQ-CT). Other end points included Global Impression Scores, and changes in body composition, behaviors, and hormones.
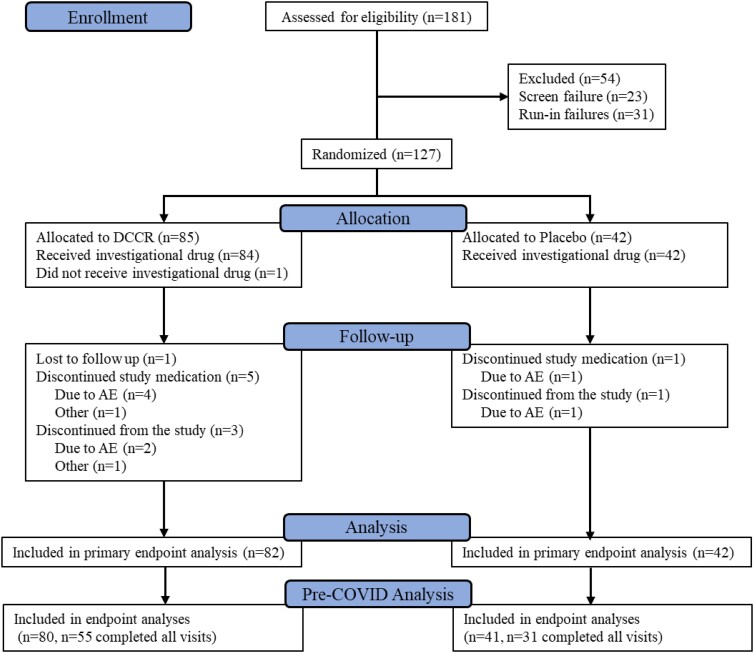
Methods: In DESTINY PWS, a 13-week, randomized, double-blind, placebo-controlled, phase 3 trial, 127 participants with PWS aged 4 years and older with hyperphagia were randomly assigned 2:1 to diazoxide choline extended-release tablet (DCCR) or placebo.
Results: DCCR did not significantly improve hyperphagia (HQ-CT least-square mean (LSmean) [SE] -5.94 [0.879] vs -4.27 [1.145]; P = .198), but did so in participants with severe hyperphagia (LSmean [SE] -9.67 [1.429] vs -4.26 [1.896]; P = .012). Two of 3 secondary end points were improved (Clinical Global Impression of Improvement [CGI-I]; P = .029; fat mass; P = .023). In an analysis of results generated pre-COVID, the primary (HQ-CT; P = .037) and secondary end points were all improved (CGI-I; P = .015; Caregiver Global Impression of Change; P = .031; fat mass; P = .003). In general, DCCR was well tolerated with 83.3% in the DCCR group experiencing a treatment-emergent adverse event and 73.8% in the placebo group (not significant).
Conclusion: DCCR did not significantly improve hyperphagia in the primary analysis but did in participants with severe baseline hyperphagia and in the pre-COVID analysis. DCCR treatment was associated with significant improvements in body composition and clinician-reported outcomes.
Trial registration: ClinicalTrials.gov NCT03440814.
Keywords: DCCR; Prader-Willi syndrome; hyperphagia.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Endocrine Society.
Conflict of interest statement
Conflict of Interest N.C. and A.B. are employed by Soleno Therapeutics and own stock in the company. N.C. is an inventor on patents assigned to Soleno Therapeutics. The institution of J.L.M., E.G., N.B., J.A.Y., P.S., K.S.O., E.I.F., L.M.B., A.H.S., M.A., M.G.B., D.S., J.A., T.B., M.L., E.L., and V.M. received funding from Soleno to support the conduct of the clinical trial. L.M.B. reports that the support provided to the organization she is associated with for the conduct of the clinical trial also included some salary support. E.G. reports receipt of lecturing and consulting fees from Soleno. J.A.Y. reports grant support from Soleno Therapeutics and from Rhythm Pharmaceuticals for obesity-related projects, and material support for research from Hikma Pharmaceuticals and Versanis-Bio.
Figures
Comment in
-
New Avenues for Pharmacological Management of Hyperphagia and Associated Behavioral Disorders in Prader-Willi Syndrome.J Clin Endocrinol Metab. 2023 Aug 18;108(9):e895-e896. doi: 10.1210/clinem/dgad131. J Clin Endocrinol Metab. 2023. PMID: 36896885 No abstract available.
References
-
- Lionti T, Reid SM, White SM, Rowell MM. A population-based profile of 160 Australians with Prader-Willi syndrome: trends in diagnosis, birth prevalence and birth characteristics. Am J Med Genet A. 2015;167A(2):371‐378. - PubMed
-
- McCandless SE. Clinical report-health supervision for children with Prader-Willi syndrome. Pediatrics. 2011;127(1):195‐204. - PubMed
