

Levofloxacin prophylaxis and parenteral nutrition have a detrimental effect on intestinal microbial networks in pediatric patients undergoing HSCT
- PMID: 36639555
- PMCID: PMC9839701
- DOI: 10.1038/s42003-023-04436-7
Levofloxacin prophylaxis and parenteral nutrition have a detrimental effect on intestinal microbial networks in pediatric patients undergoing HSCT
Abstract
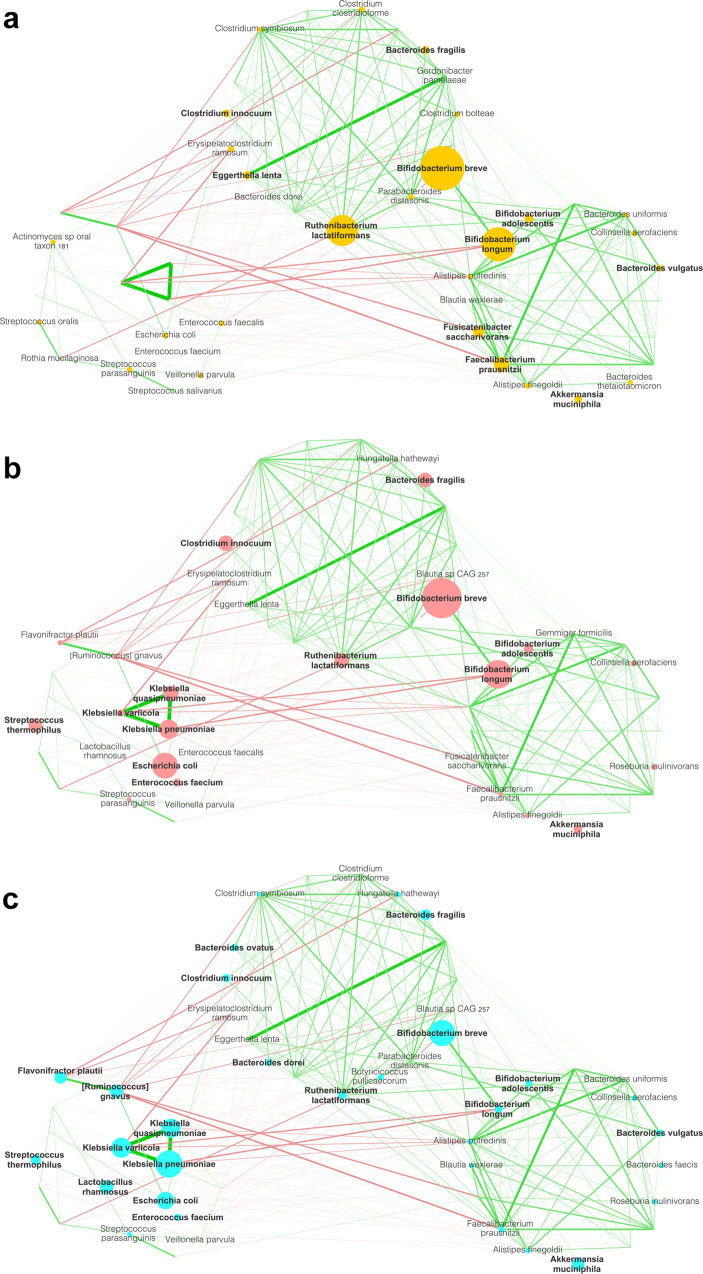
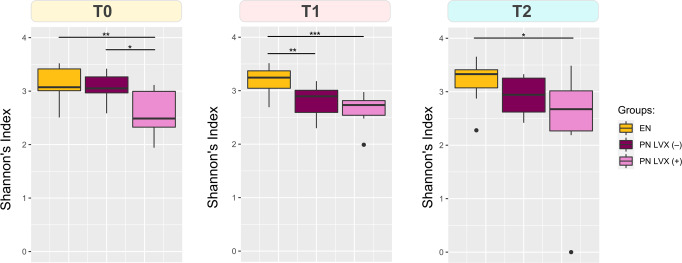
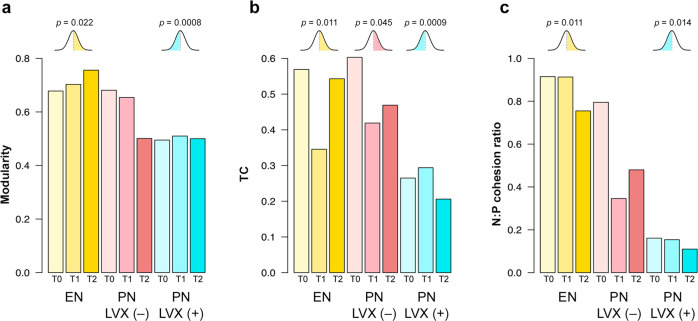
The gut microbiome (GM) has shown to influence hematopoietic stem cell transplantation (HSCT) outcome. Evidence on levofloxacin (LVX) prophylaxis usefulness before HSCT in pediatric patients is controversial and its impact on GM is poorly characterized. Post-HSCT parenteral nutrition (PN) is oftentimes the first-line nutritional support in the neutropenic phase, despite the emerging benefits of enteral nutrition (EN). In this exploratory work, we used a global-to-local networking approach to obtain a high-resolution longitudinal characterization of the GM in 30 pediatric HSCT patients receiving PN combined with LVX prophylaxis or PN alone or EN alone. By evaluating the network topology, we found that PN, especially preceded by LVX prophylaxis, resulted in a detrimental effect over the GM, with low modularity, poor cohesion, a shift in keystone species and the emergence of modules comprising several pathobionts, such as Klebsiella spp., [Ruminococcus] gnavus, Flavonifractor plautii and Enterococcus faecium. Our pilot findings on LVX prophylaxis and PN-related disruption of GM networks should be considered in patient management, to possibly facilitate prompt recovery/maintenance of a healthy and well-wired GM. However, the impact of LVX prophylaxis and nutritional support on short- to long-term post-HSCT clinical outcomes has yet to be elucidated.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
