

Pediatric trauma and emergency surgery: an international cross-sectional survey among WSES members
- PMID: 36639810
- PMCID: PMC9840264
- DOI: 10.1186/s13017-022-00473-5
Pediatric trauma and emergency surgery: an international cross-sectional survey among WSES members
Abstract
Background: In contrast to adults, the situation for pediatric trauma care from an international point of view and the global management of severely injured children remain rather unclear. The current study investigates structural management of pediatric trauma in centers of different trauma levels as well as experiences with pediatric trauma management around the world.
Methods: A web-survey had been distributed to the global mailing list of the World Society of Emergency Surgery from 10/2021-03/2022, investigating characteristics of respondents and affiliated hospitals, case-load of pediatric trauma patients, capacities and infrastructure for critical care in children, trauma team composition, clinical work-up and individual experiences with pediatric trauma management in response to patients´ age. The collaboration group was subdivided regarding sizes of affiliated hospitals to allow comparisons concerning hospital volumes. Comparable results were conducted to statistical analysis.
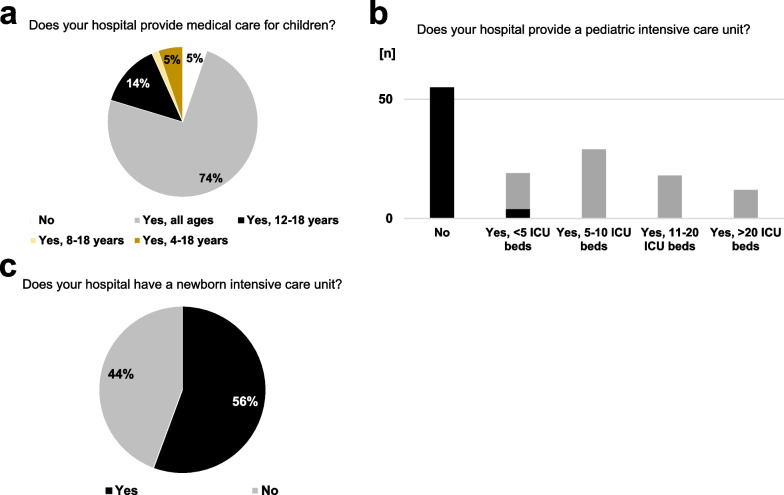
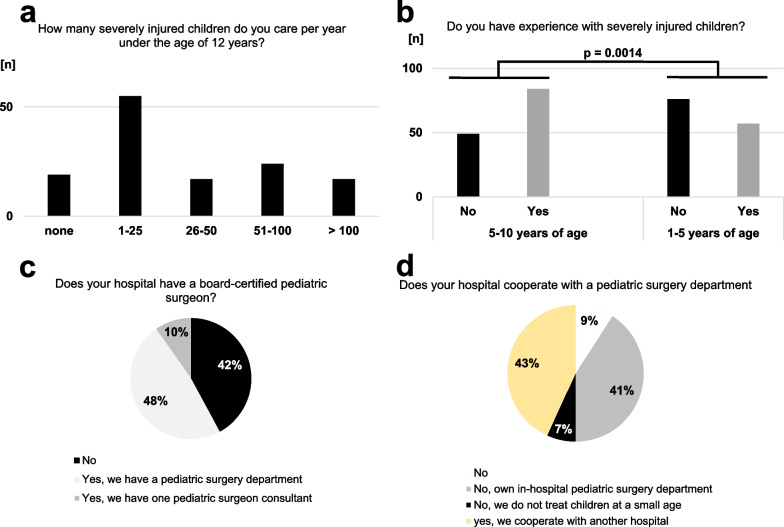
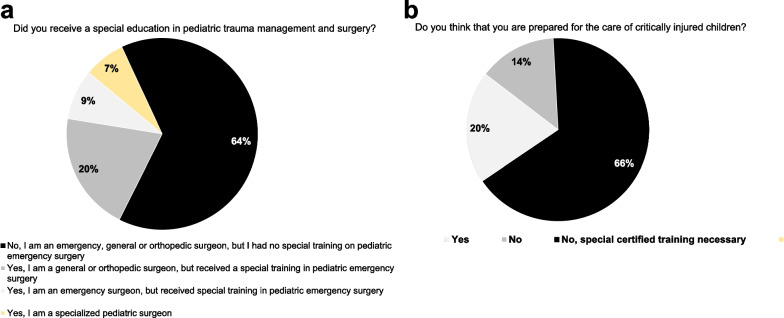
Results: A total of 133 participants from 34 countries, i.e. 5 continents responded to the survey. They were most commonly affiliated with larger hospitals (> 500 beds in 72.9%) and with level I or II trauma centers (82.0%), respectively. 74.4% of hospitals offer unrestricted pediatric medical care, but only 63.2% and 42.9% of the participants had sufficient experiences with trauma care in children ≤ 10 and ≤ 5 years of age (p = 0.0014). This situation is aggravated in participants from smaller hospitals (p < 0.01). With regard to hospital size (≤ 500 versus > 500 in-hospital beds), larger hospitals were more likely affiliated with advanced trauma centers, more elaborated pediatric intensive care infrastructure (p < 0.0001), treated children at all ages more frequently (p = 0.0938) and have higher case-loads of severely injured children < 12 years of age (p = 0.0009). Therefore, the majority of larger hospitals reserve either pediatric surgery departments or board-certified pediatric surgeons (p < 0.0001) and in-hospital trauma management is conducted more multi-disciplinarily. However, the majority of respondents does not feel prepared for treatment of severe pediatric trauma and call for special educational and practical training courses (overall: 80.2% and 64.3%, respectively).
Conclusions: Multi-professional management of pediatric trauma and individual experiences with severely injured children depend on volumes, level of trauma centers and infrastructure of the hospital. However, respondents from hospitals at all levels of trauma care complain about an alarming lack of knowledge on pediatric trauma management.
Keywords: Appendicitis; Children; Emergency; Emergency surgery; Injury; Pediatric surgery; Pediatric trauma; Trauma surgery; WSES.
© 2023. The Author(s).
Conflict of interest statement
None declared.
Figures


References
-
- Bouillon B. S3 – Leitlinie Polytrauma/Schwerverletztenbehandlung, AWMF Register-Nr. 012/019. 2016;
-
- Schmittenbecher PP. S2k - Leitlinie Polytraumaversorgung im Kindesalter, AWMF Register-Nr. 006–120. 2020;
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
