

CEST-MRI for body oncologic imaging: are we there yet?
- PMID: 36640112
- PMCID: PMC10200773
- DOI: 10.1002/nbm.4906
CEST-MRI for body oncologic imaging: are we there yet?
Abstract
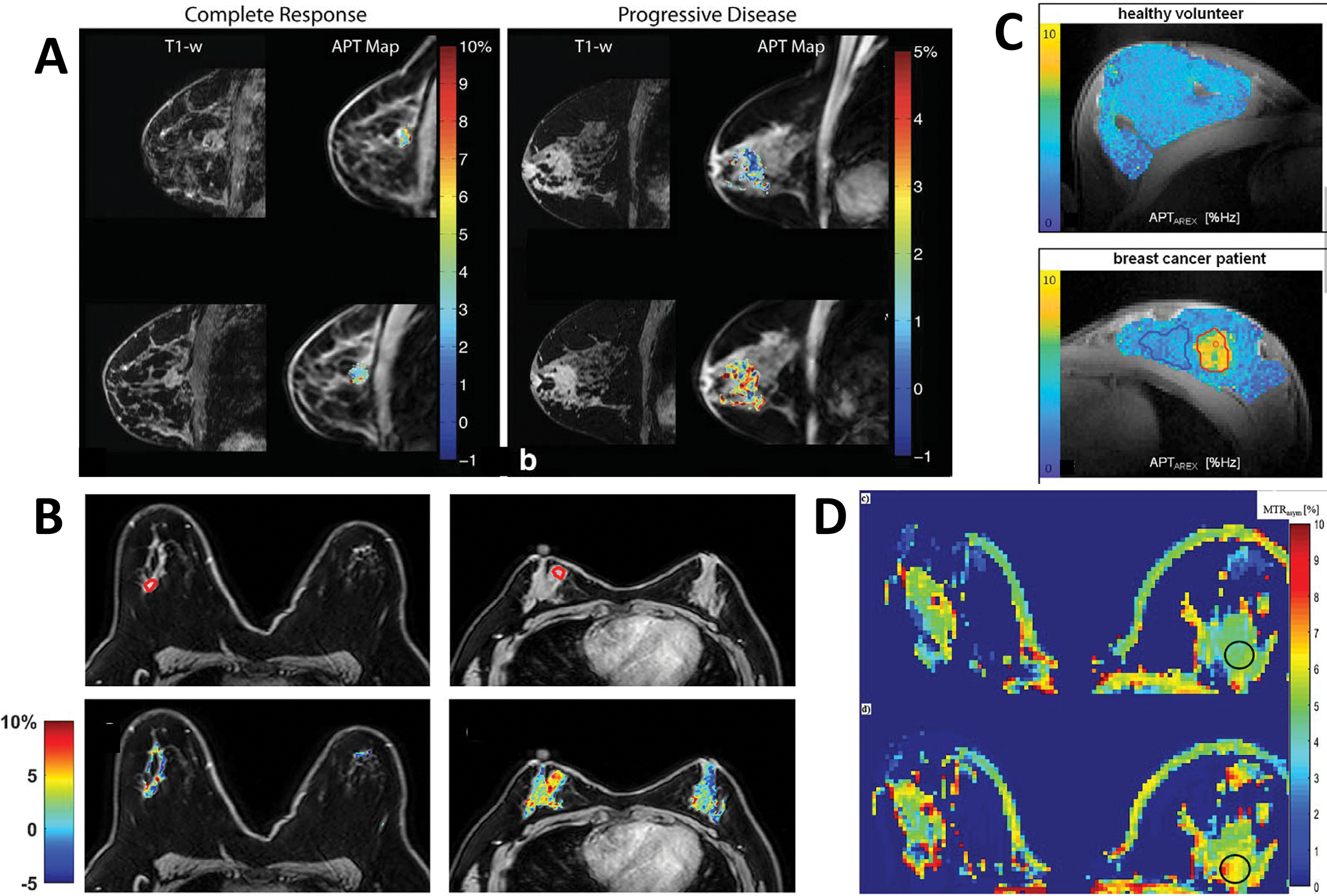
Chemical exchange saturation transfer (CEST) MRI has gained recognition as a valuable addition to the molecular imaging and quantitative biomarker arsenal, especially for characterization of brain tumors. There is also increasing interest in the use of CEST-MRI for applications beyond the brain. However, its translation to body oncology applications lags behind those in neuro-oncology. The slower migration of CEST-MRI to non-neurologic applications reflects the technical challenges inherent to imaging of the torso. In this review, we discuss the application of CEST-MRI to oncologic conditions of the breast and torso (i.e., body imaging), emphasizing the challenges and potential solutions to address them. While data are still limited, reported studies suggest that CEST signal is associated with important histology markers such as tumor grade, receptor status, and proliferation index, some of which are often associated with prognosis and response to therapy. However, further technical development is still needed to make CEST a reliable clinical application for body imaging and establish its role as a predictive and prognostic biomarker.
Keywords: APT; CEST; MRI; body imaging; oncologic imaging.
© 2023 John Wiley & Sons, Ltd.
Figures






References
-
- Hagiwara A, Tatekawa H, Yao J, et al. Visualization of tumor heterogeneity and prediction of isocitrate dehydrogenase mutation status for human gliomas using multiparametric physiologic and metabolic MRI. Article. Scientific Reports. 2022;12(1)1078. doi:10.1038/s41598-022-05077-2 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
