

Validation of a semi-automatic method to measure total liver volumes in polycystic liver disease on computed tomography - high speed and accuracy
- PMID: 36640173
- PMCID: PMC10121488
- DOI: 10.1007/s00330-022-09346-6
Validation of a semi-automatic method to measure total liver volumes in polycystic liver disease on computed tomography - high speed and accuracy
Abstract
Objectives: Polycystic liver disease (PLD) is characterized by growth of hepatic cysts, causing hepatomegaly. Disease severity is determined using total liver volume (TLV), which can be measured from computed tomography (CT). The gold standard is manual segmentation which is time-consuming and requires expert knowledge of the anatomy. This study aims to validate the commercially available semi-automatic MMWP (Multimodality Workplace) Volume tool for CT scans of PLD patients.
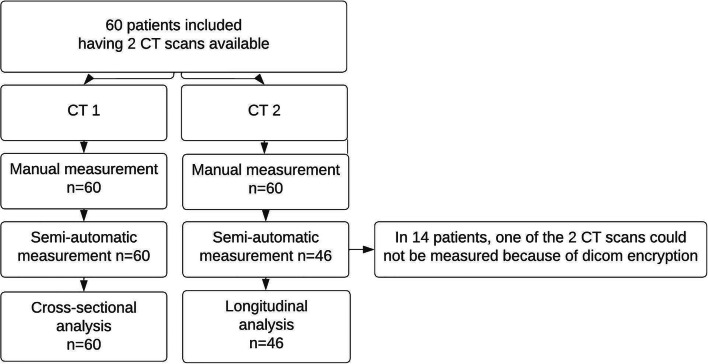
Methods: We included adult patients with one (n = 60) or two (n = 46) abdominal CT scans. Semi-automatic contouring was compared with manual segmentation, using comparison of observed volumes (cross-sectional) and growth (longitudinal), correlation coefficients (CC), and Bland-Altman analyses with bias and precision, defined as the mean difference and SD from this difference. Inter- and intra-reader variability were assessed using coefficients of variation (CV) and we assessed the time to perform both procedures.
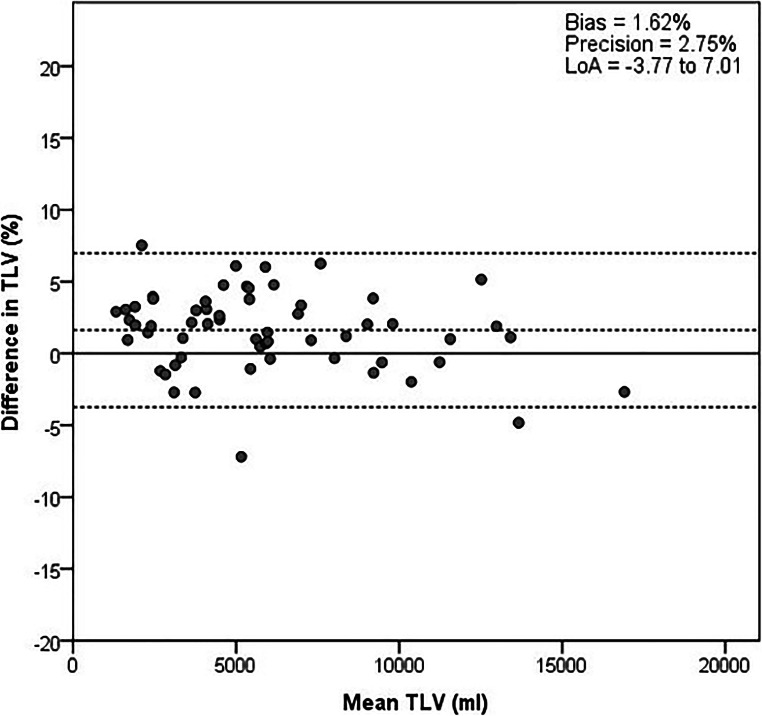
Results: Median TLV was 5292.2 mL (IQR 3141.4-7862.2 mL) at baseline. Cross-sectional analysis showed high correlation and low bias and precision between both methods (CC 0.998, bias 1.62%, precision 2.75%). Absolute volumes were slightly higher for semi-automatic segmentation (manual 5292.2 (3141.4-7862.2) versus semi-automatic 5432.8 (3071.9-7960.2) mL, difference 2.7%, p < 0.001). Longitudinal analysis demonstrated that semi-automatic segmentation accurately measures liver growth (CC 0.908, bias 0.23%, precision 4.04%). Inter- and intra-reader variability were small (2.19% and 0.66%) and comparable to manual segmentation (1.21% and 0.63%) (p = 0.26 and p = 0.37). Semi-automatic segmentation was faster than manual tracing (19 min versus 50 min, p = 0.009).
Conclusions: Semi-automatic liver segmentation is a fast and accurate method to determine TLV and liver growth in PLD patients.
Key points: • Semi-automatic liver segmentation using the commercially available MMWP volume tool accurately determines total liver volume as well as liver growth over time in polycystic liver disease patients. • This method is considerably faster than manual segmentation through the use of Hounsfield unit settings. • We used a real-life CT set for the validation and showed that the semi-automatic tool measures accurately regardless of contrast used for the CT scan or not, presence of polycystic kidneys, liver volume, and previous invasive treatment for polycystic liver disease.
Keywords: Organ size; Polycystic kidney disease; Polycystic liver disease; Radiology; Tomography, X-ray computed.
© 2023. The Author(s).
Conflict of interest statement
The authors of this manuscript declare relationships with the following companies: Dr. Drenth has received grant support from Abbvie and Gilead. Dr. Gansevoort received grant support and fees for serving on advisory boards and steering committees from Galapagos, IPSEN, Otsuka Pharmaceuticals, and Sanofi-Genzyme. In addition, Dr. Gansevoort holds the Orphan Medicinal Product Designation status at the European Medicines Agency for lanreotide as treatment for kidney function decline in ADPKD (EMA/OD/027/15). All money is paid to their institutions. No other potential conflict of interest relevant to this article was reported.
No grants have a relation with the current study.
Figures


References
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
