

Prostate cancer lesion detection, volume quantification and high-grade cancer differentiation using cancer risk maps derived from multiparametric MRI with histopathology as the reference standard
- PMID: 36641104
- PMCID: PMC11229728
- DOI: 10.1016/j.mri.2023.01.006
Prostate cancer lesion detection, volume quantification and high-grade cancer differentiation using cancer risk maps derived from multiparametric MRI with histopathology as the reference standard
Abstract
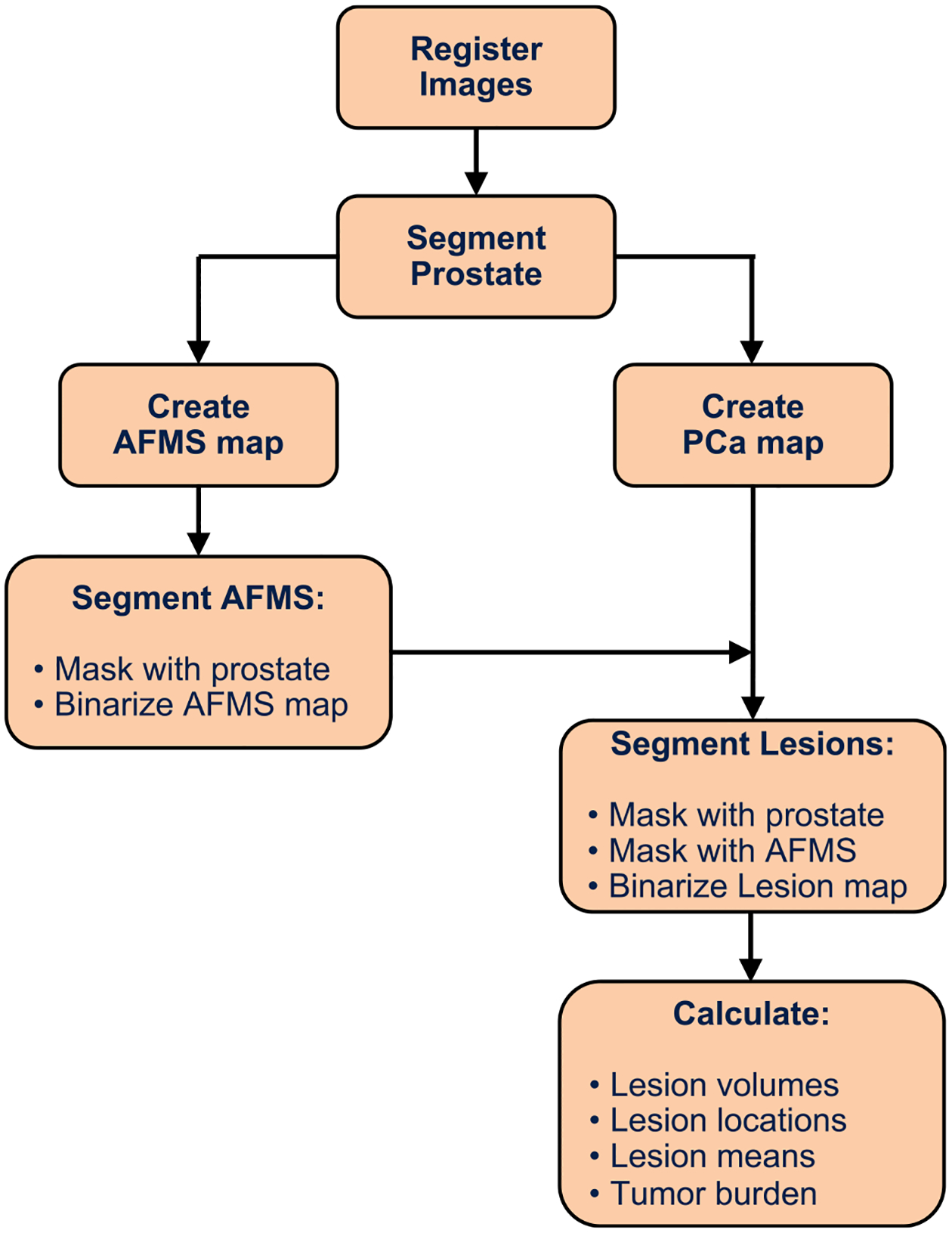
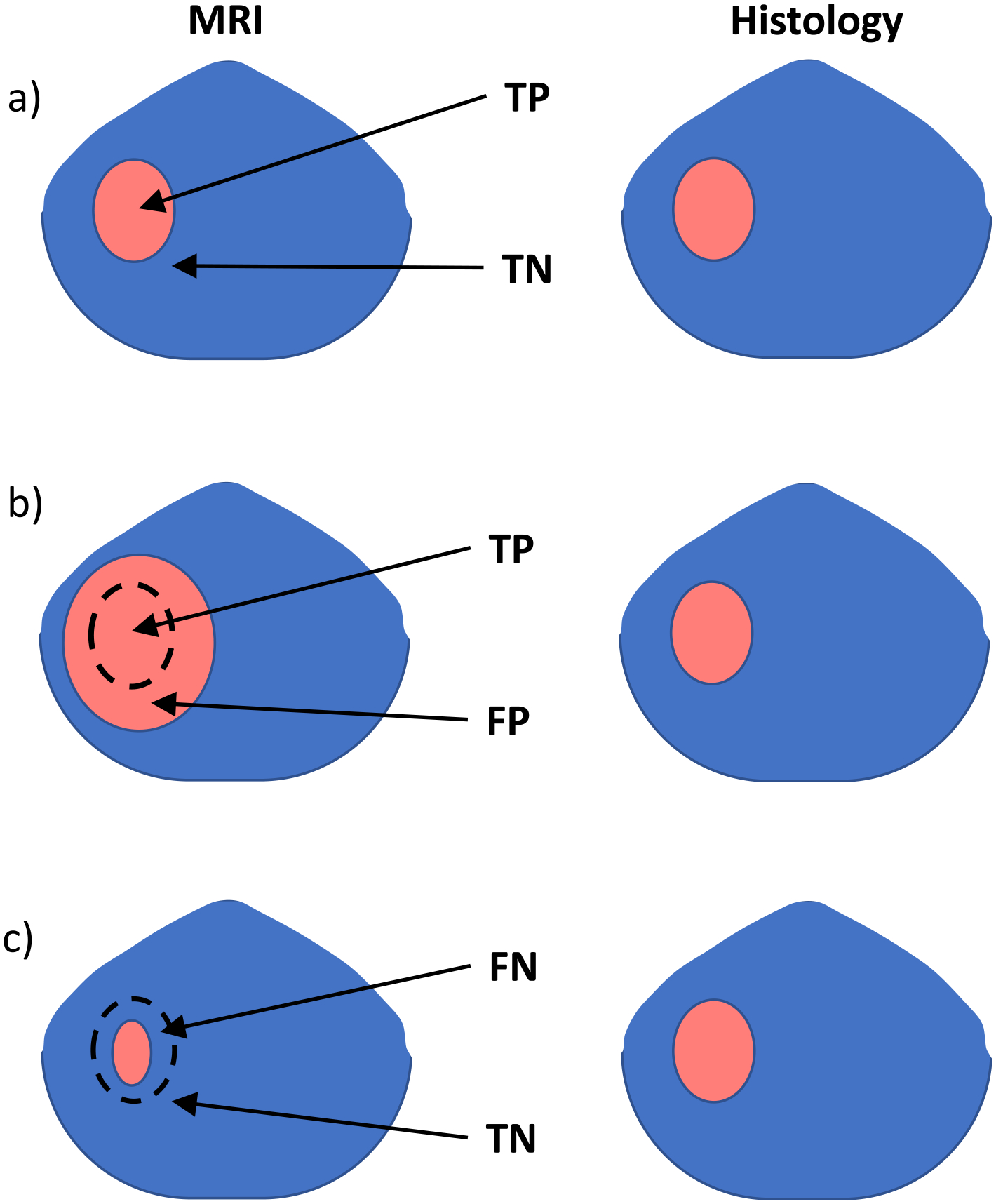
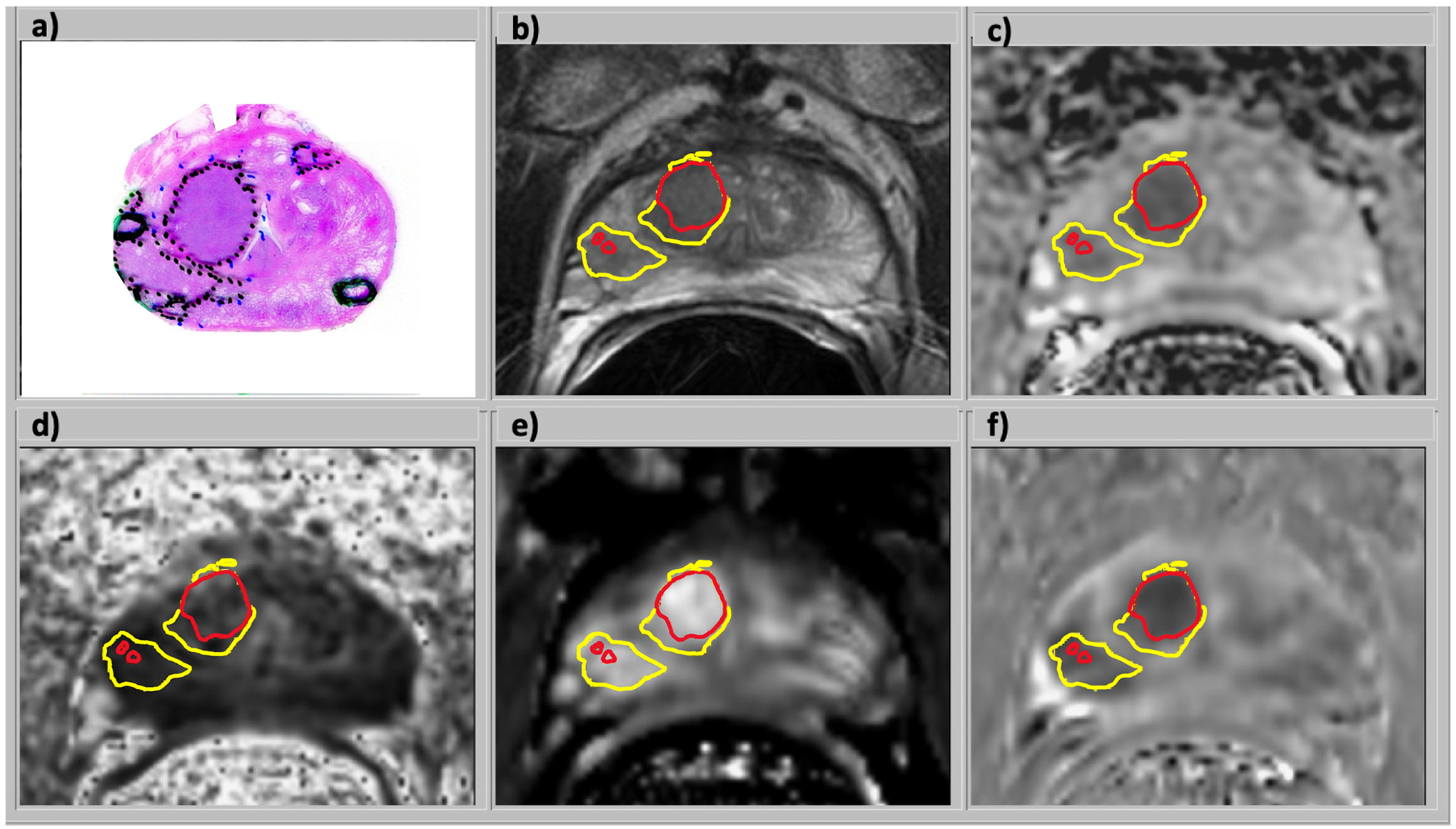
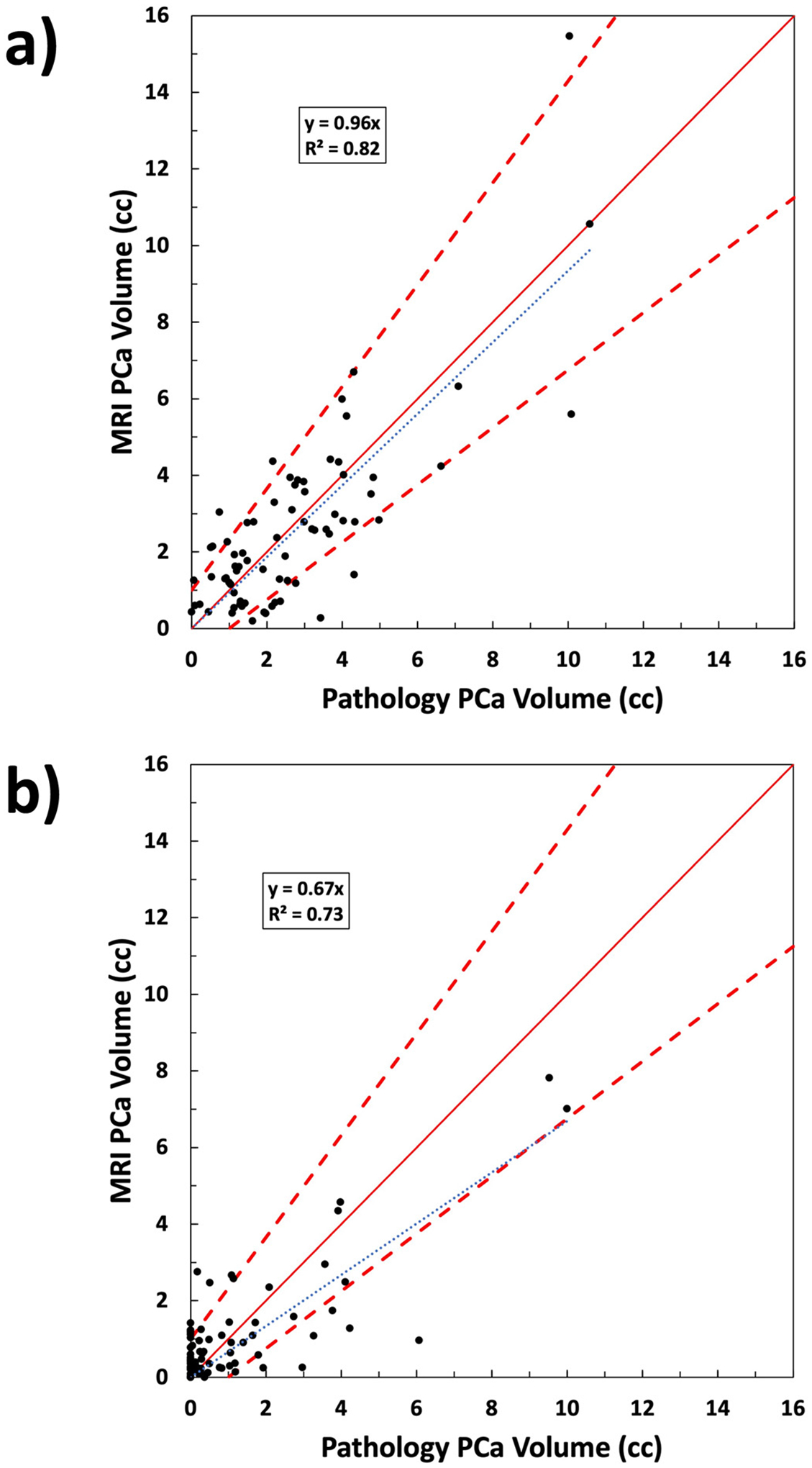
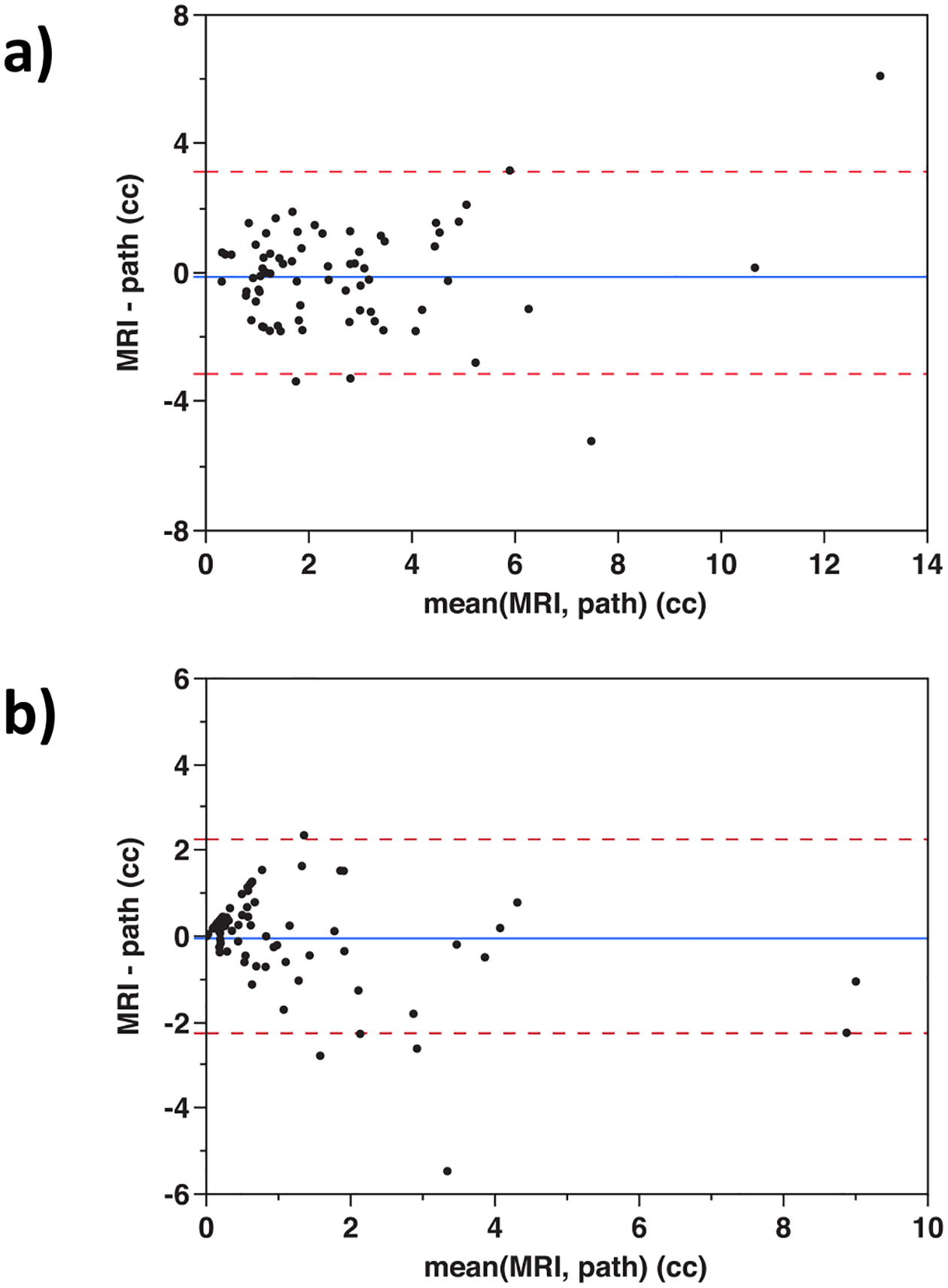
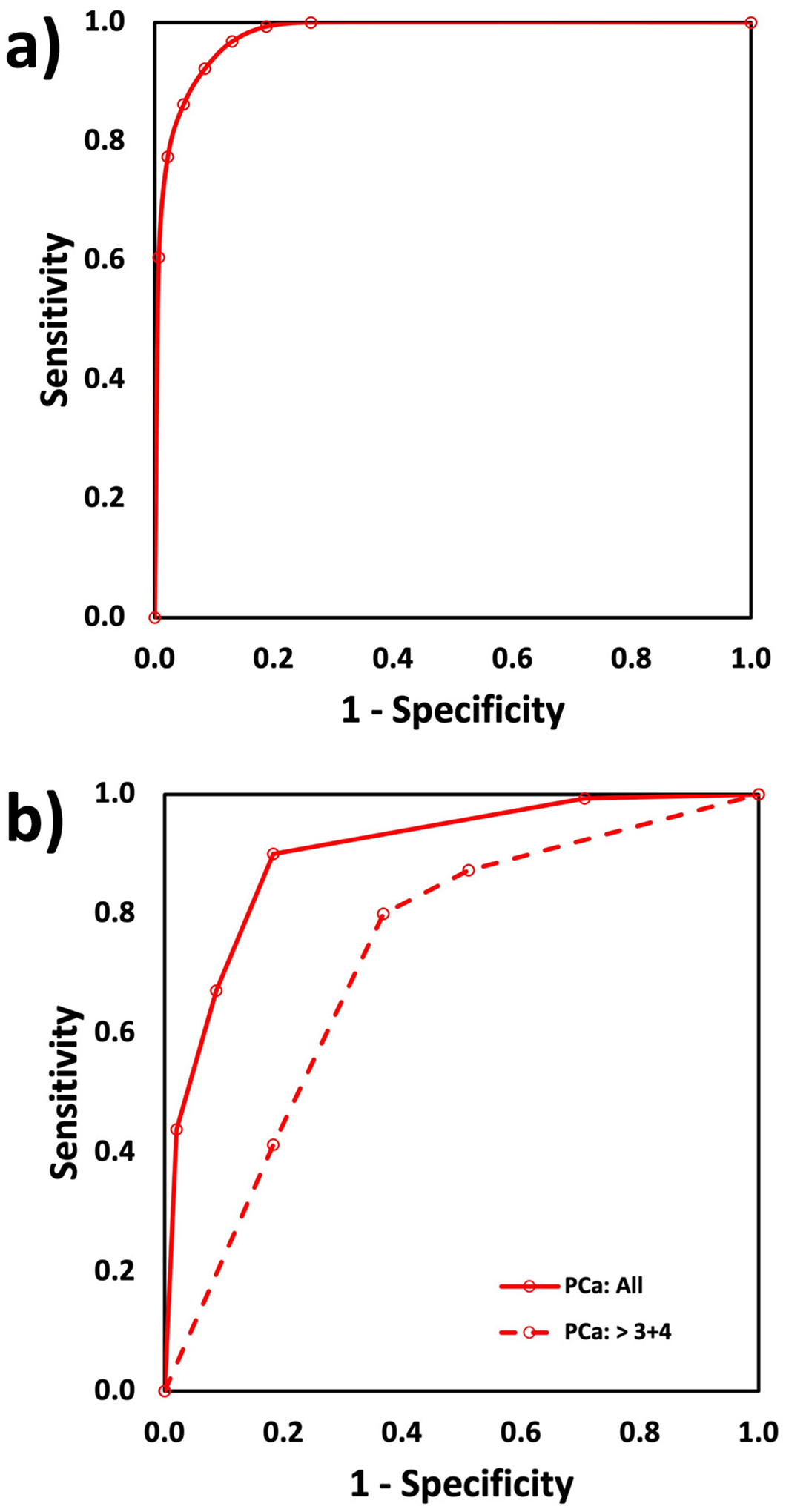
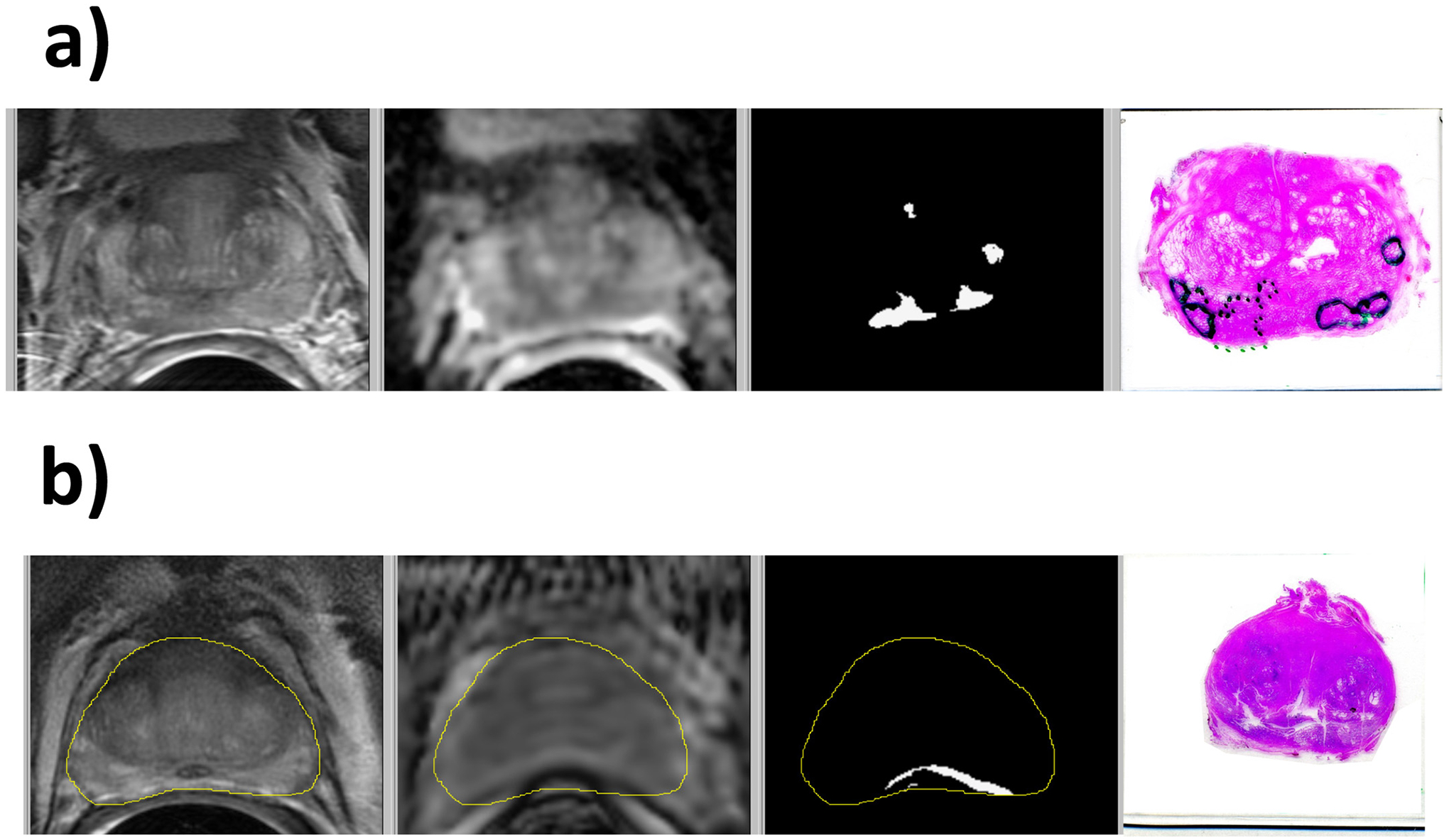
Multi-parametric MRI (mpMRI) has proven itself a clinically useful tool to assess prostate cancer (PCa). Our objective was to generate PCa risk maps to quantify the volume and location of both all PCa and high grade (Gleason grade group ≥ 3) PCa. Such capabilities would aid physicians and patients in treatment decisions, targeting biopsy, and planning focal therapy. A cohort of men with biopsy proven prostate cancer and pre-prostatectomy mpMRI were studied. PCa and benign ROIs (1524) were identified on mpMRI and histopathology with histopathology serving as the reference standard. Logistic regression models were created to differentiate PCa from benign tissues. The MRI images were registered to ensure correct overlay. The cancer models were applied to each image voxel within prostates to create probability maps of cancer and of high-grade cancer. Use of an optimum probability threshold quantified PCa volume for all lesions >0.1 cc. Accuracies were calculated using area under the curve (AUC) for the receiver operating characteristic (ROC). The PCa models utilized apparent diffusion coefficient (ADC), T2 weighted (T2W), dynamic contrast-enhanced MRI (DCE MRI) enhancement slope, and DCE MRI washout as the statistically significant MRI scans. Application of the PCa maps method provided total PCa volume and individual lesion volumes. The AUCs derived from lesion analysis were 0.91 for all PCa and 0.73 for high-grade PCa. At the optimum threshold, the PCa maps detected 135 / 150 (90%) histopathological lesions >0.1 cc. This study showed the feasibility of cancer risk maps, created from pre-prostatectomy, mpMR images validated with histopathology, to detect PCa lesions >0.1 cc. The method quantified the volume of cancer within the prostate. Method improvements were identified by determining root causes for over and underestimation of cancer volumes. The maps have the potential for improved non-invasive capability in quantitative detection, localization, volume estimation, and MRI characterization of PCa.
Keywords: Diffusion-weighted imaging; Dynamic contrast-enhanced imaging; Histopathology; Multiparametric MRI; Prostate cancer.
Copyright © 2023 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest None.
Figures
References
-
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin 2022;72:7–33. - PubMed
