

Association between total cholesterol and total bone mineral density in US adults: National Health and Nutrition Examination Survey (NHANES), 2011-2018
- PMID: 36642708
- PMCID: PMC9841665
- DOI: 10.1186/s13018-022-03485-8
Association between total cholesterol and total bone mineral density in US adults: National Health and Nutrition Examination Survey (NHANES), 2011-2018
Abstract
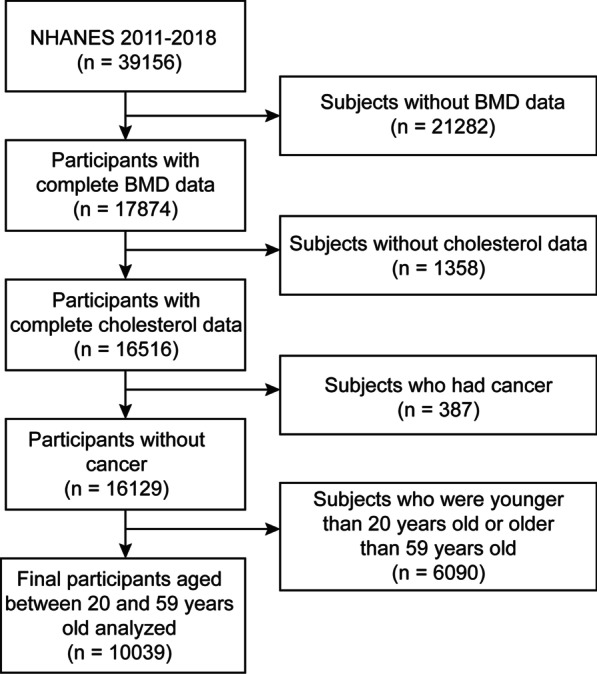
Background: Accumulated evidence indicates that cholesterol is offensive to bone metabolism. Therefore, we examined the real-world study among total cholesterol and total bone mineral density (BMD). We investigated the relationship between total cholesterol and total BMD among 10,039 US participants aged 20-59 years old over the period 2011-2018 from the NHANES.
Methods: To analyze the relationship among total cholesterol and total BMD, multivariate linear regression models were used. Fitted smoothing curves, generalized additive models, and threshold effect analysis were also conducted.
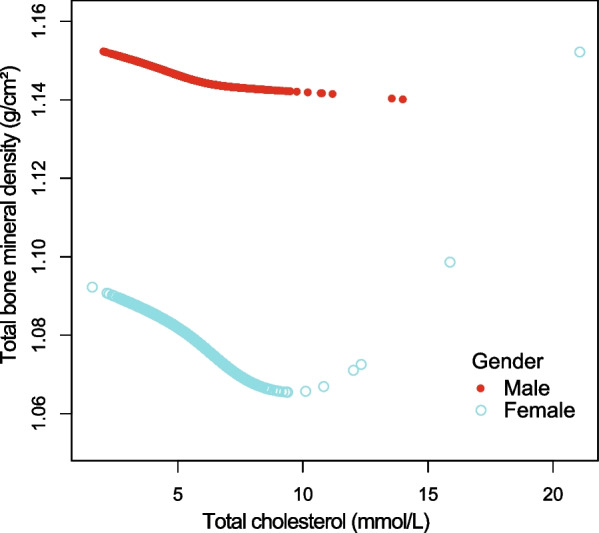
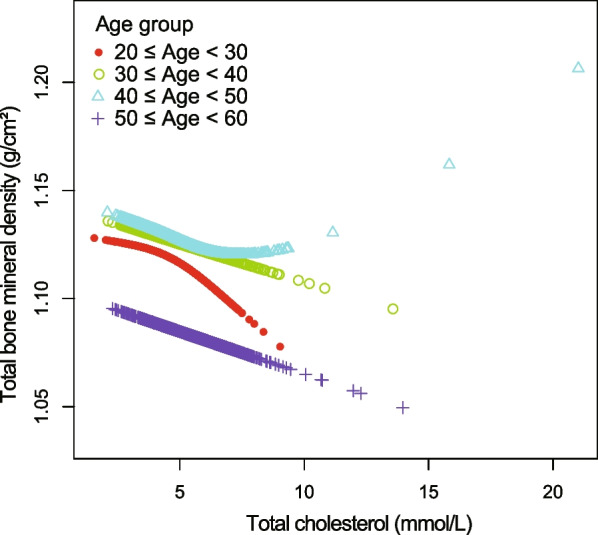
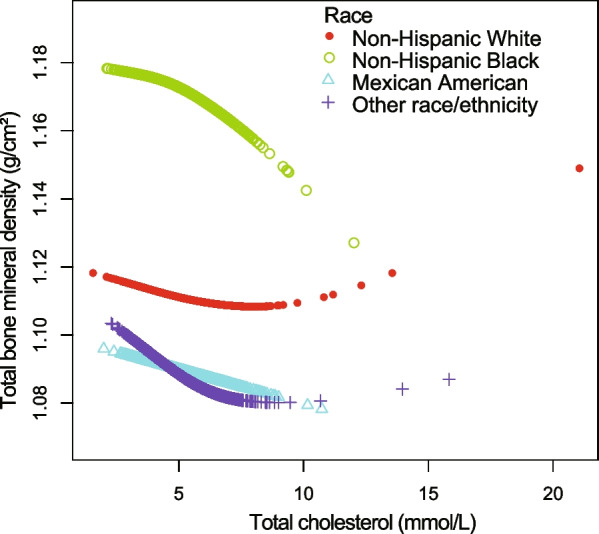
Results: After adjusting for additional covariates, weighted multivariable linear regression models indicated total cholesterol concentration levels exhibited a negative relationship with total BMD, particularly among participants aged 20-29 years. Concerning subgroup analysis, stratified by gender, race/ethnicity and age group, the negative correlation of total cholesterol with total BMD dwelled in both female and male as well as in whites and other races (including Hispanic and Multi-Racial), but not in non-Hispanic blacks and Mexican American. In other races, this relationship presented a nonlinear association (inflection point: 6.7 mmol/L) with a U-shaped curve. Among participants aged 40 to 49 years, this relationship also followed a nonlinear association (inflection point: 5.84 mmol/L), indicating a saturation effect. Moreover, the three types of diabetes status were found to have negative, U-shaped, and positive relationships. In participants with borderline diabetes status, the relationship of total cholesterol with total BMD was a U-shaped curve (inflection point: 4.65 mmol/L).
Conclusions: For US young adults (20-29 years old), our study revealed a negative relationship between total cholesterol and total BMD. This association followed a U-shaped curve (inflection point: 4.65 mmol/L) in borderline diabetes status participants, a saturation curve (inflection point: 5.84 mmol/L) in participants aged 40-49 years and a nonlinear curve (inflection point: 6.7 mmol/L) in other races (including Hispanic and Multi-Racial). Therefore, keeping total cholesterol concentration at a reasonable level for young adults and diabetic population might be an approach to prevent osteoporosis or osteopenia.
Keywords: Bone mineral density; Cholesterol; Osteopenia; Osteoporosis.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
