

Association of growth differentiation factor-15 level with adverse outcomes in patients with stable coronary artery disease: A meta-analysis
- PMID: 36643602
- PMCID: PMC9833259
- DOI: 10.1016/j.athplu.2021.11.003
Association of growth differentiation factor-15 level with adverse outcomes in patients with stable coronary artery disease: A meta-analysis
Abstract
Background and aims: Studies on the association between growth-differentiation factor-15 (GDF-15) level and adverse outcomes have yielded conflicting results in patients with stable coronary artery disease (CAD). This meta-analysis aimed to evaluate the association of baseline GDF-15 level with adverse outcomes in stable CAD patients.
Methods: Two authors independently searched PubMed and Embase databases from inception to May 31, 2021 for available studies that investigated the association of baseline GDF-15 level with all-cause mortality, cardiovascular mortality, or major adverse cardiovascular events (MACEs) in stable CAD patients. Pooled multivariable adjusted hazard ratio (HR) with 95% confidence interval (CI) was calculated for the highest vs. the lowest GDF-15 level.
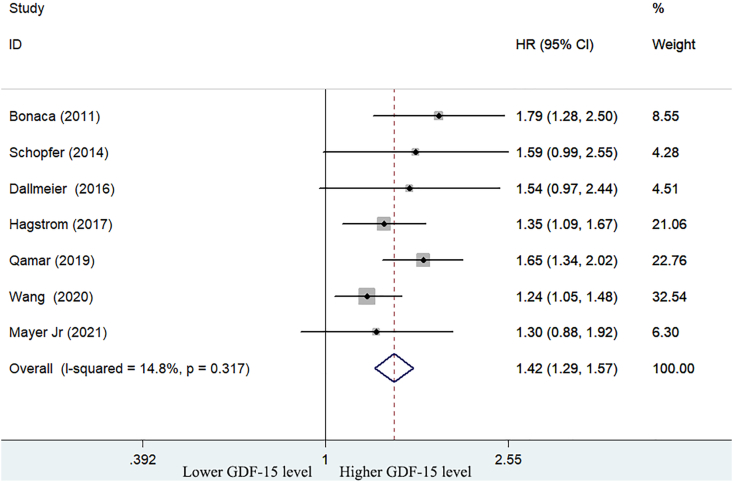
Results: Seven studies that involved 28,765 stable CAD patients were identified and analyzed. The meta-analysis showed that the highest GDF-15 level was associated with higher risk of MACEs (HR 1.42; 95% CI 1.29-1.57; p < 0.001), cardiovascular mortality (HR 1.64: 95% CI 1.25-2.14; p < 0.001), and all-cause mortality (HR 2.01; 95% CI 1.67-2.42; p < 0.001) when compared the lowest GDF-15 level. Moreover, the values of GDF-15 level in predicting MACEs were consistently observed in each named subgroup.
Conclusions: Elevated blood GDF-15 level is an independent predictor of MACEs, cardiovascular mortality, and all-cause mortality in stable CAD patients. The baseline GDF-15 level may play an important role in the risk stratification of stable CAD patients.
Keywords: Growth-differentiation factor-15; Major adverse cardiovascular events; Meta-analysis; Mortality; Stable coronary artery disease.
© 2021 The Authors.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Figures




Similar articles
-
Predictive value of baseline C-reactive protein level in patients with stable coronary artery disease: A meta-analysis.Medicine (Baltimore). 2022 Sep 2;101(35):e30285. doi: 10.1097/MD.0000000000030331. Medicine (Baltimore). 2022. PMID: 36107517 Free PMC article.
-
Growth differentiation factor-15 is associated with cardiovascular outcomes in patients with coronary artery disease.Cardiovasc Diabetol. 2020 Aug 3;19(1):120. doi: 10.1186/s12933-020-01092-7. Cardiovasc Diabetol. 2020. PMID: 32746821 Free PMC article.
-
Prognostic Value of Baseline d-Dimer Level in Patients With Coronary Artery Disease: A Meta-Analysis.Angiology. 2022 Jan;73(1):18-25. doi: 10.1177/00033197211019805. Epub 2021 Jun 3. Angiology. 2022. PMID: 34078130
-
Prognostic value of growth differentiation factor-15 in patients with coronary artery disease: A meta-analysis and systematic review.Front Cardiovasc Med. 2023 Feb 10;10:1054187. doi: 10.3389/fcvm.2023.1054187. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 36844747 Free PMC article.
-
Prognostic value of asymmetric dimethylarginine in patients with coronary artery disease: A meta-analysis.Nitric Oxide. 2021 May 1;109-110:50-56. doi: 10.1016/j.niox.2021.03.002. Epub 2021 Mar 6. Nitric Oxide. 2021. PMID: 33684543 Review.
Cited by
-
Inflammatory and vascular biomarkers as predictors of all-cause death and cardiovascular outcomes in an Australian community-based cohort.Physiol Rep. 2025 Jun;13(11):e70379. doi: 10.14814/phy2.70379. Physiol Rep. 2025. PMID: 40495286 Free PMC article.
-
GDF-15 is a potential candidate biomarker for an elevated risk of cardiotoxicity in breast cancer patients receiving neoadjuvant dual anti-HER2 therapy.Front Pharmacol. 2024 May 17;15:1396133. doi: 10.3389/fphar.2024.1396133. eCollection 2024. Front Pharmacol. 2024. PMID: 38828460 Free PMC article.
References
-
- Fox K.A.A., Metra M., Morais J., Atar D. The myth of 'stable' coronary artery disease. Nat Rev Cardiol. 2020;17:9–21. - PubMed
-
- Braun M.M., Stevens W.A., Barstow C.H. Stable coronary artery disease: treatment. Am Fam Physician. 2018;97:376–384. - PubMed
-
- Ruiz Ortiz M., Ogayar C., Romo E., Mesa D., Delgado M., Anguita M., et al. Long-term survival in elderly patients with stable coronary disease. Eur J Clin Invest. 2013;43:774–782. - PubMed
-
- Vidal-Petiot E., Ford I., Greenlaw N., Ferrari R., Fox K.M., Tardif J.C., et al. Cardiovascular event rates and mortality according to achieved systolic and diastolic blood pressure in patients with stable coronary artery disease: an international cohort study. Lancet. 2016;388:2142–2152. - PubMed
-
- McCarthy C.P., McEvoy J.W., Januzzi J.L., Jr. Biomarkers in stable coronary artery disease. Am Heart J. 2018;196:82–96. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous