

Urinary pteridines as a discriminator of atherosclerotic risk in patients with diabetes
- PMID: 36643725
- PMCID: PMC9833246
- DOI: 10.1016/j.athplu.2021.11.001
Urinary pteridines as a discriminator of atherosclerotic risk in patients with diabetes
Abstract
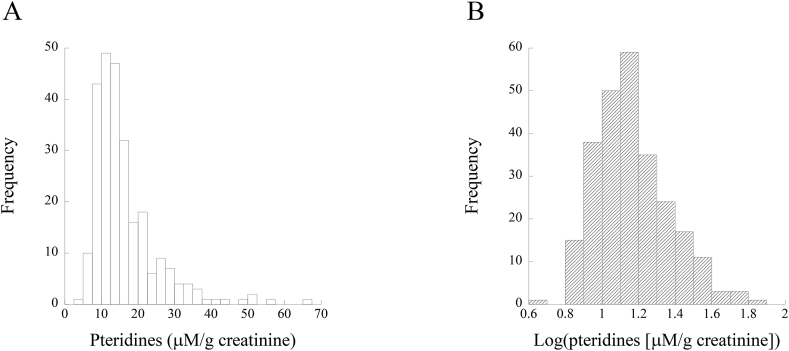
Background and aims: We have recently proposed urinary pteridine level as a useful biomarker of oxidative stress in a general population. However, the significance of urinary pteridines in patients with diabetes is unknown.
Methods: The relationships of the level of urinary pteridine derivatives with d-dimer, ankle-brachial pressure index (ABI), and known cardiovascular risk factors were investigated in patients with type 2 diabetes.
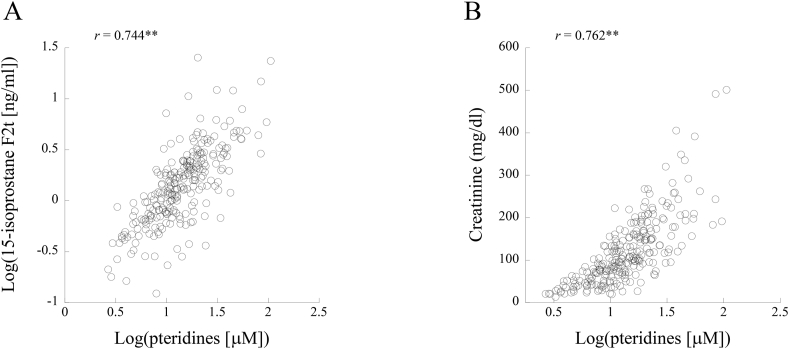
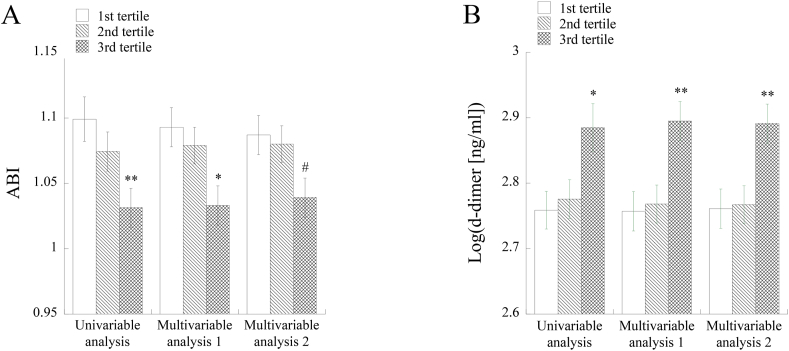
Results: Urinary pteridine level showed significant positive correlations with urinary15-isoprostane F2t, female gender, history of smoking and d-dimer and significant inverse correlations with history of alcohol drinking, body mass index (BMI) and ABI. ABI was significantly lower and d-dimer was significantly higher in the highest tertile group of pteridines than in the lowest tertile group. The odds ratios of the highest vs. lowest tertiles for low ABI and high d-dimer were significantly higher than the reference level. The above relationships of urinary pteridines with ABI and d-dimer were not altered when age, gender, BMI, hemoglobin A1c and history of alcohol drinking were used as explanatory variables in multivariable analyses. History of smoking confounded the relation of pteridines with ABI but not that with d-dimer. However, in logistic regression analysis, the association between pteridines and ABI remained significant with adjustment for history of smoking.
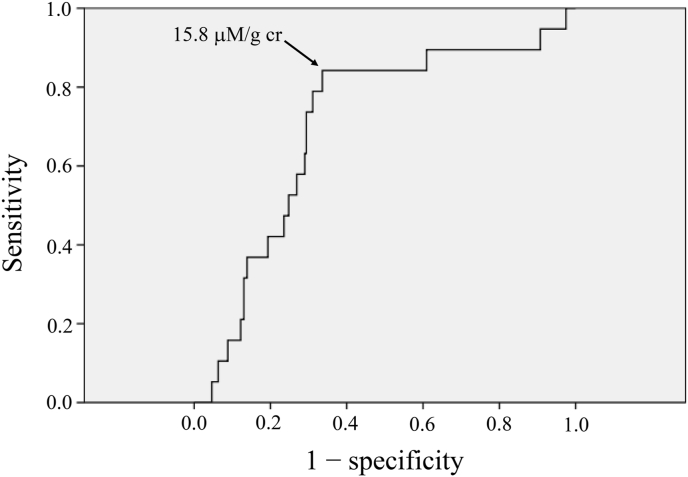
Conclusion: Urinary pteridine level was associated with d-dimer and ABI, which reflect blood coagulability and arterial flow to the lower extremities, respectively, and is thus thought to be a useful discriminator of thromboatherosclerotic risk in patients with diabetes.
Keywords: Blood coagulation; Diabetes; Oxidative stress; Peripheral arterial disease; Pteridines.
© 2021 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Gu K., Cowie C.C., Harris M.I. Mortality in adults with and without diabetes in a national cohort of the U.S. population, 1971-1993. Diabetes Care. 1998;21:1138–1145. - PubMed
-
- Gao X., Song J., Watase H., Hippe D.S., Zhao X., et al. Differences in carotid plaques between symptomatic patients with and without diabetes mellitus. Arterioscler Thromb Vasc Biol. 2019;39:1234–1239. CARE-II Investigators. - PubMed
-
- Low Wang C.C., Hess C.N., Hiatt W.R., Goldfine A.B. Clinical update: cardiovascular disease in diabetes mellitus: atherosclerotic cardiovascular disease and heart failure in Type 2 diabetes mellitus - mechanisms, management, and clinical considerations. Circulation. 2016;133:2459–2502. - PMC - PubMed
LinkOut - more resources
Full Text Sources