

Impact of atherosclerotic extent on clinical outcome for diabetic patients with non-obstructive coronary artery disease
- PMID: 36644667
- PMCID: PMC9833230
- DOI: 10.1016/j.athplu.2021.07.021
Impact of atherosclerotic extent on clinical outcome for diabetic patients with non-obstructive coronary artery disease
Abstract
Background and aims: The prognostic impact of non-obstructive coronary artery disease (CAD) has long been underestimated due to its mild stenosis (<50% stenosis). We aim to investigate the prognostic value of atherosclerotic extent in DM patients with non-obstructive CAD.
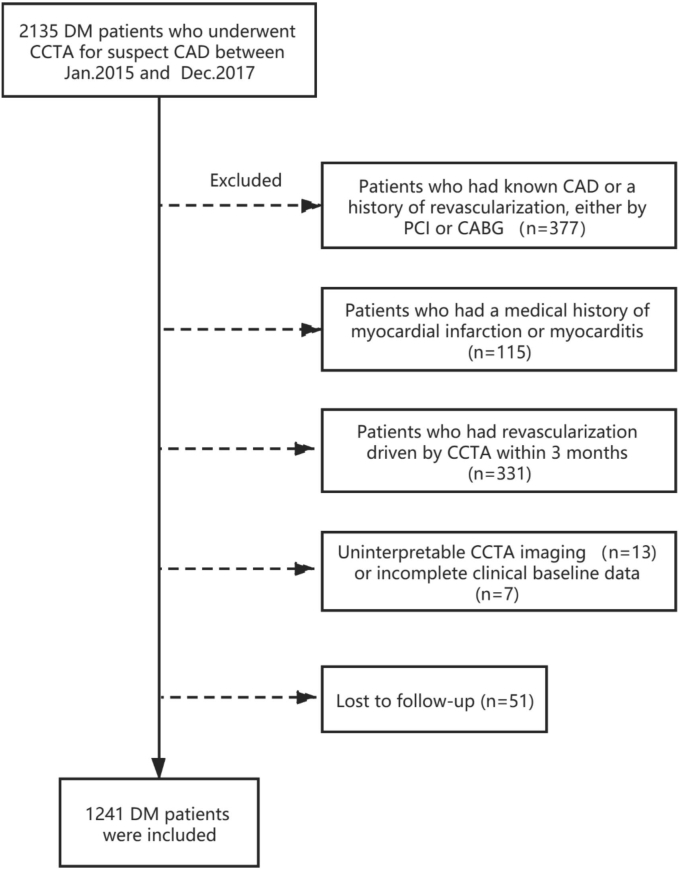
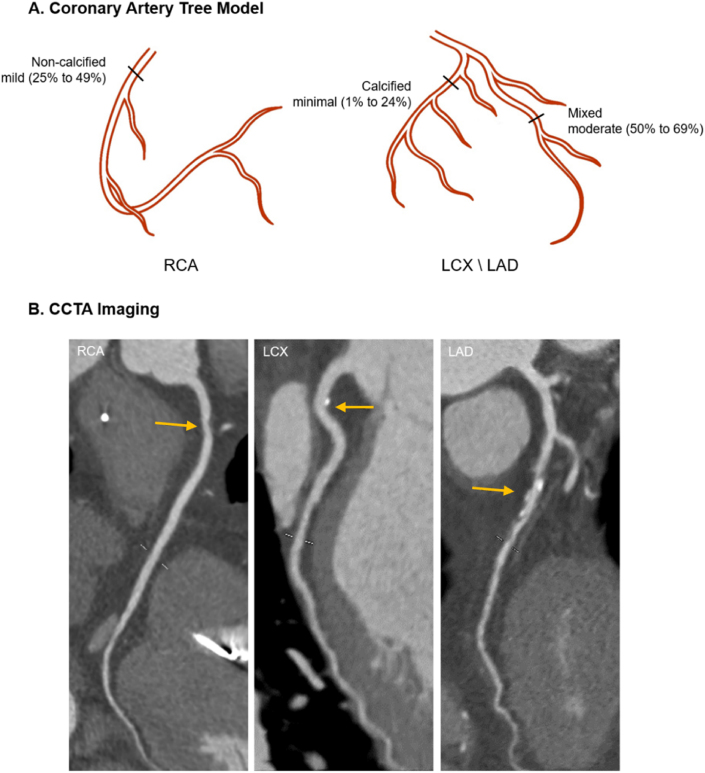
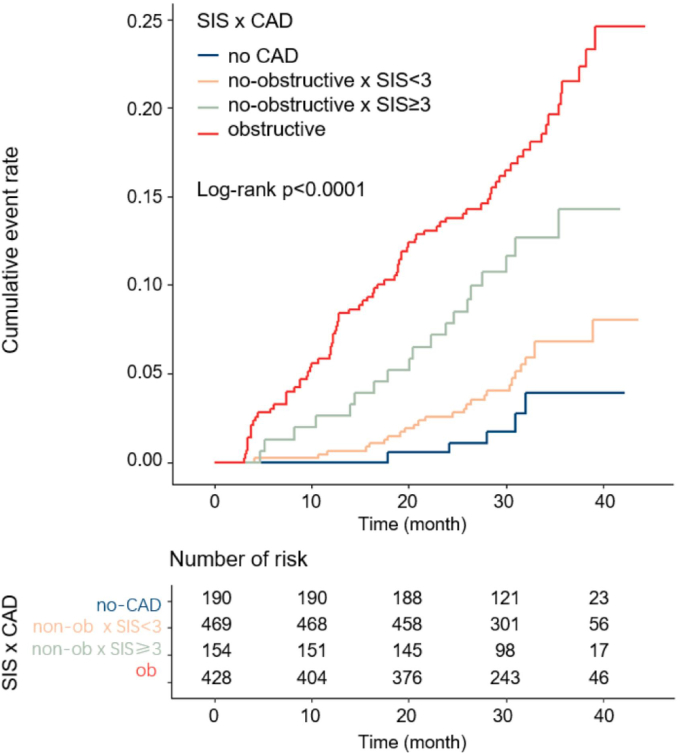
Methods: The analysis was based on a single center cohort of DM patients referred for coronary computed tomography angiography (CCTA) due to suspect CAD in 2015-2017. Based on coronary stenosis combined with segment involvement score (SIS), the study population were divided into four groups: normal (0% stenosis), non-obstructive SIS<3, non-obstructive SIS≥3 and obstructive (≥50% stenosis). The intra-class correlation (ICC) was used to test the inter-and intra-reviewer agreement. Multivariate Cox model and Kaplan-Meier method were used to evaluate the effect size of atherosclerotic extent on the prognosis.
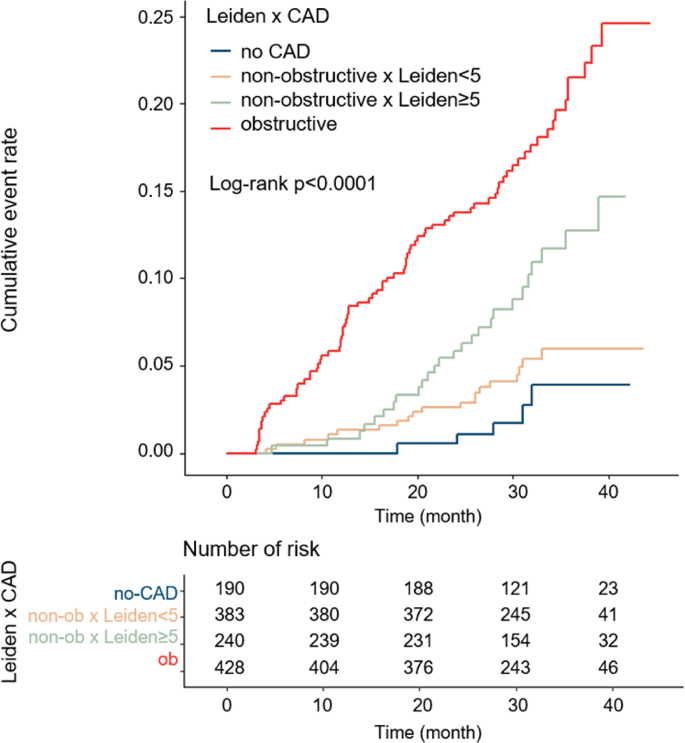
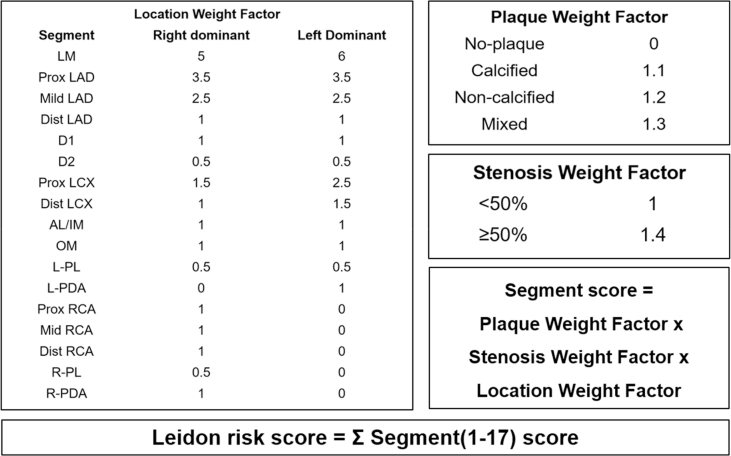
Results: In total, 1241 patients (age 60.2 ± 10.4 years, 54.1% male) were included, of which 50.2% were non-obstructive. During a median follow-up of 2.6 years, 131 MACEs (10.6%) were adjudicated, including 17 cardiovascular deaths, 28 non-fatal myocardial infarctions, 64 unstable anginas requiring hospitalization and 22 strokes. Incremental event rates could be observed across the four groups. After adjustment for age, gender, hyperlipidemia and presence of high-risk plaque, Hazard Ratio (HR) for non-obstructive SIS<3, non-obstructive SIS≥3 and the obstructive group was 1.84 (95%CI: 0.70-4.79), 3.71 (95%CI: 1.37-10.00) and 5.46 (95%CI: 2.18-13.69), respectively. Compared with non-obstructive SIS<3, non-obstructive SIS≥3 showed a significantly higher risk (HR:2.02 95%CI:1.11-3.68, p = 0.021). Similar results were demonstrated when Leiden risk score was used for sensitivity analysis.
Conclusion: In DM patients with non-obstructive CAD, atherosclerotic extent was associated with higher risk of major adverse cardiac events at long-term follow-up. Efforts should be made to determine risk stratification for the management of DM patients with non-obstructive CAD.
Keywords: Atherosclerosis; Coronary computed tomography angiography; Diabetes mellitus; Non-obstructive coronary artery disease; Risk stratification.
© 2021 6th Medical Center of Chinese PLA General Hospital.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Lee K.Y., Hwang B.H., Kim T.H., Kim C.J., Kim J.J., Choo E.H., Choi I.J., Choi Y., Park H.W., Koh Y.S., et al. Computed tomography angiography images of coronary artery stenosis provide a better prediction of risk than traditional risk factors in asymptomatic individuals with type 2 diabetes: a long-term study of clinical outcomes. Diabetes Care. 2017;40(9):1241–1248. - PubMed
-
- Blanke P., Naoum C., Ahmadi A., Cheruvu C., Soon J., Arepalli C., Gransar H., Achenbach S., Berman D.S., Budoff M.J., et al. Long-term prognostic utility of coronary CT angiography in stable patients with diabetes mellitus. JACC Cardiovasc Imag. 2016;9(11):1280–1288. - PubMed
-
- Radico F., Zimarino M., Fulgenzi F., Ricci F., Di Nicola M., Jespersen L., Chang S.M., Humphries K.H., Marzilli M., De Caterina R. Determinants of long-term clinical outcomes in patients with angina but without obstructive coronary artery disease: a systematic review and meta-analysis. Eur Heart J. 2018;39(23):2135–2146. - PubMed
-
- Investigators S.-H., Newby D.E., Adamson P.D., Berry C., Boon N.A., Dweck M.R., Flather M., Forbes J., Hunter A., Lewis S., et al. Coronary CT angiography and 5-year risk of myocardial infarction. N Engl J Med. 2018;379(10):924–933. - PubMed
-
- van Rosendael A.R., Bax A.M., Smit J.M., van den Hoogen I.J., Ma X., Al'Aref S., Achenbach S., Al-Mallah M.H., Andreini D., Berman D.S., et al. Clinical risk factors and atherosclerotic plaque extent to define risk for major events in patients without obstructive coronary artery disease: the long-term coronary computed tomography angiography CONFIRM registry. Eur Heart J Cardiovasc Imag. 2020;21(5):479–488. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous