

Model to predict major complications following liver resection for HCC in patients with metabolic syndrome
- PMID: 36646670
- PMCID: PMC10121838
- DOI: 10.1097/HEP.0000000000000027
Model to predict major complications following liver resection for HCC in patients with metabolic syndrome
Abstract
Background: Metabolic syndrome (MS) is rapidly growing as risk factor for HCC. Liver resection for HCC in patients with MS is associated with increased postoperative risks. There are no data on factors associated with postoperative complications.
Aims: The aim was to identify risk factors and develop and validate a model for postoperative major morbidity after liver resection for HCC in patients with MS, using a large multicentric Western cohort.
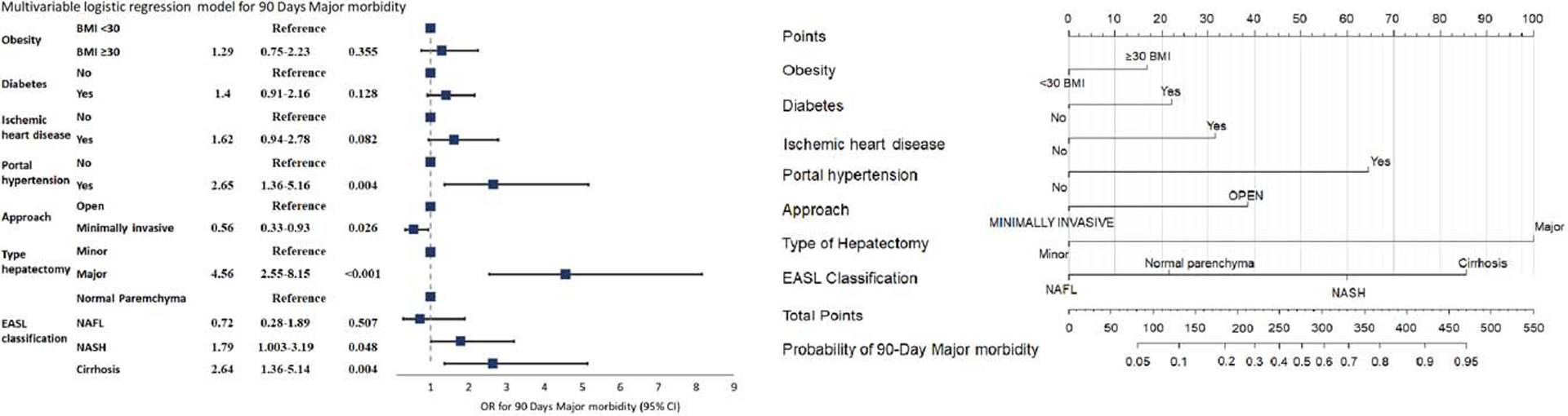
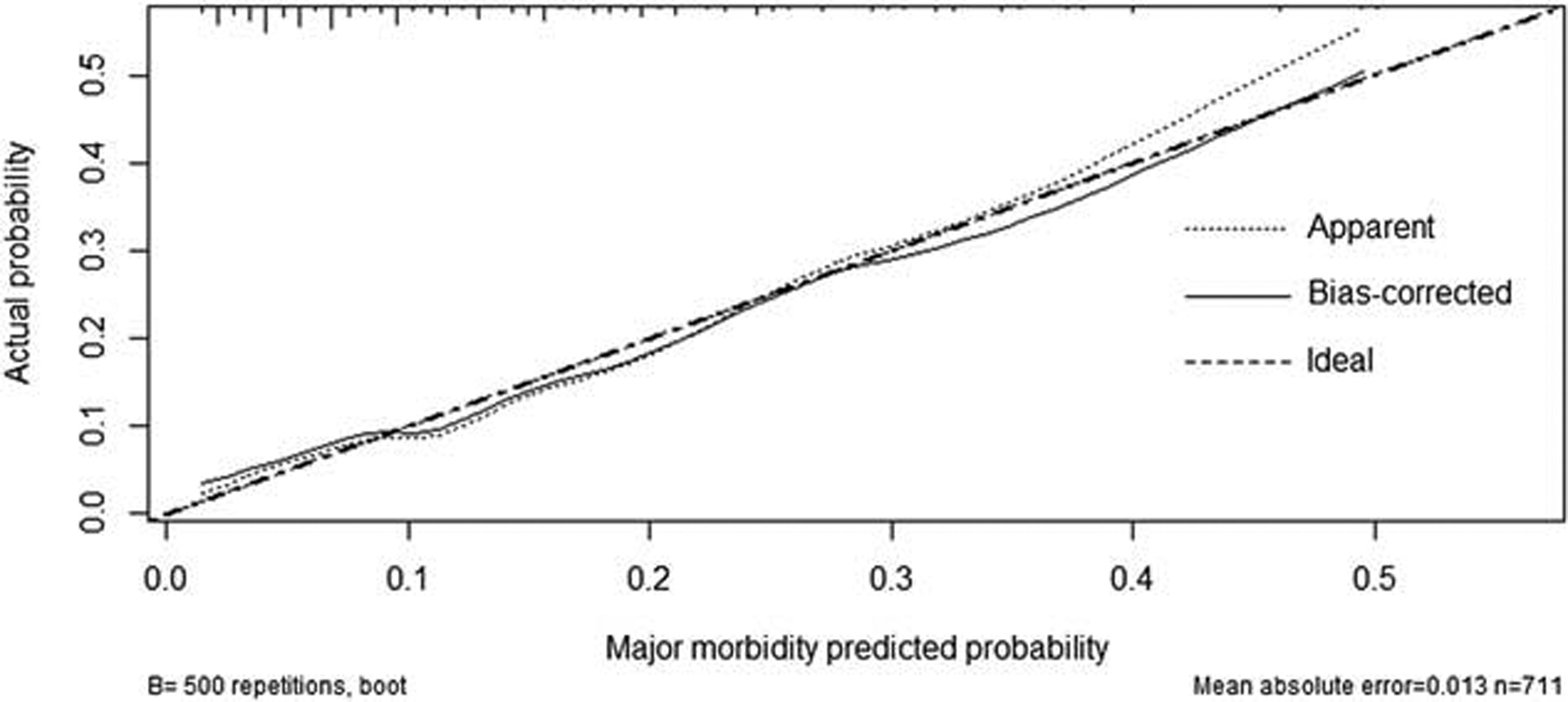
Materials and methods: The univariable logistic regression analysis was applied to select predictive factors for 90 days major morbidity. The model was built on the multivariable regression and presented as a nomogram. Performance was evaluated by internal validation through the bootstrap method. The predictive discrimination was assessed through the concordance index.
Results: A total of 1087 patients were gathered from 24 centers between 2001 and 2021. Four hundred and eighty-four patients (45.2%) were obese. Most liver resections were performed using an open approach (59.1%), and 743 (68.3%) underwent minor hepatectomies. Three hundred and seventy-six patients (34.6%) developed postoperative complications, with 13.8% major morbidity and 2.9% mortality rates. Seven hundred and thirteen patients had complete data and were included in the prediction model. The model identified obesity, diabetes, ischemic heart disease, portal hypertension, open approach, major hepatectomy, and changes in the nontumoral parenchyma as risk factors for major morbidity. The model demonstrated an AUC of 72.8% (95% CI: 67.2%-78.2%) ( https://childb.shinyapps.io/NomogramMajorMorbidity90days/ ).
Conclusions: Patients undergoing liver resection for HCC and MS are at high risk of postoperative major complications and death. Careful patient selection, considering baseline characteristics, liver function, and type of surgery, is key to achieving optimal outcomes.
Copyright © 2023 American Association for the Study of Liver Diseases.
Figures
Comment in
-
Liver resection for HCC in patients with metabolic syndrome: questions answered, questions raised.Hepatology. 2023 May 1;77(5):1463-1464. doi: 10.1097/HEP.0000000000000034. Epub 2023 Jan 3. Hepatology. 2023. PMID: 36645223 No abstract available.
References
-
- Agopian VG, Kaldas FM, Hong JC, et al. Liver transplantation for nonalcoholic steatohepatitis: the new epidemic. Ann Surg. 2012; 256:624–33. - PubMed
-
- European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J Hepatol. 2018;69:182–236. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
