

[11C]metomidate PET-CT versus adrenal vein sampling for diagnosing surgically curable primary aldosteronism: a prospective, within-patient trial
- PMID: 36646800
- PMCID: PMC9873572
- DOI: 10.1038/s41591-022-02114-5
[11C]metomidate PET-CT versus adrenal vein sampling for diagnosing surgically curable primary aldosteronism: a prospective, within-patient trial
Abstract
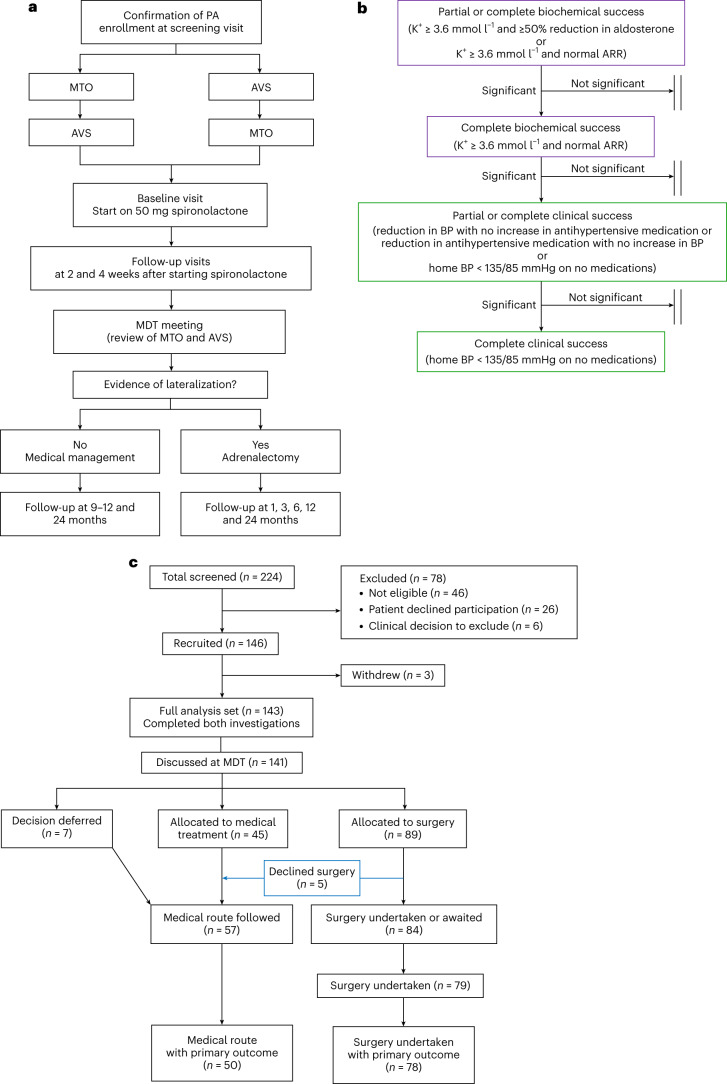
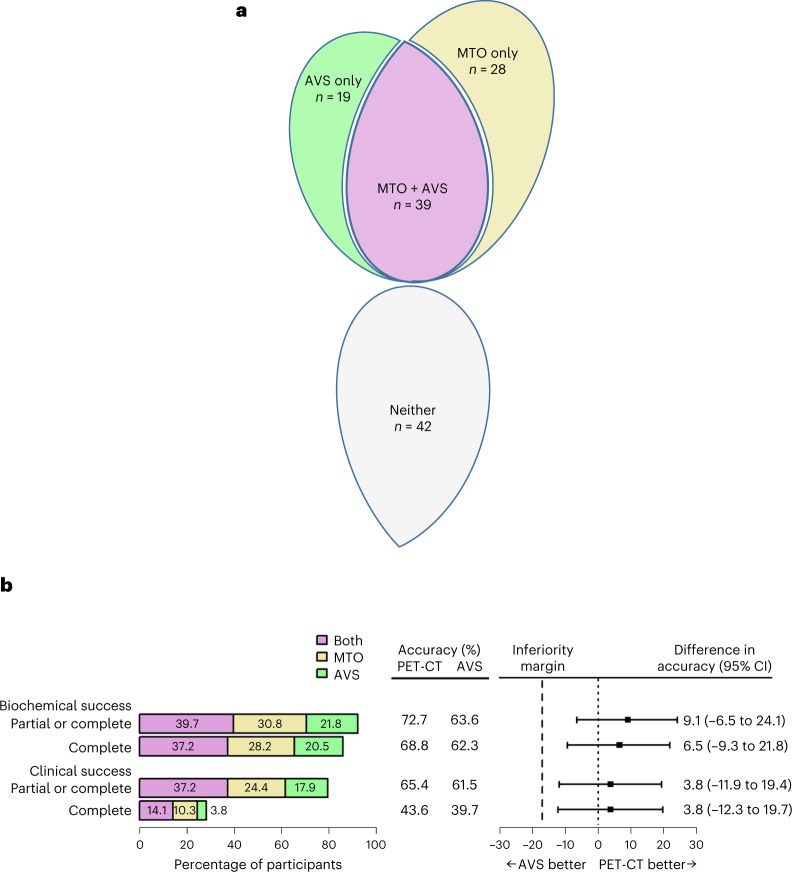
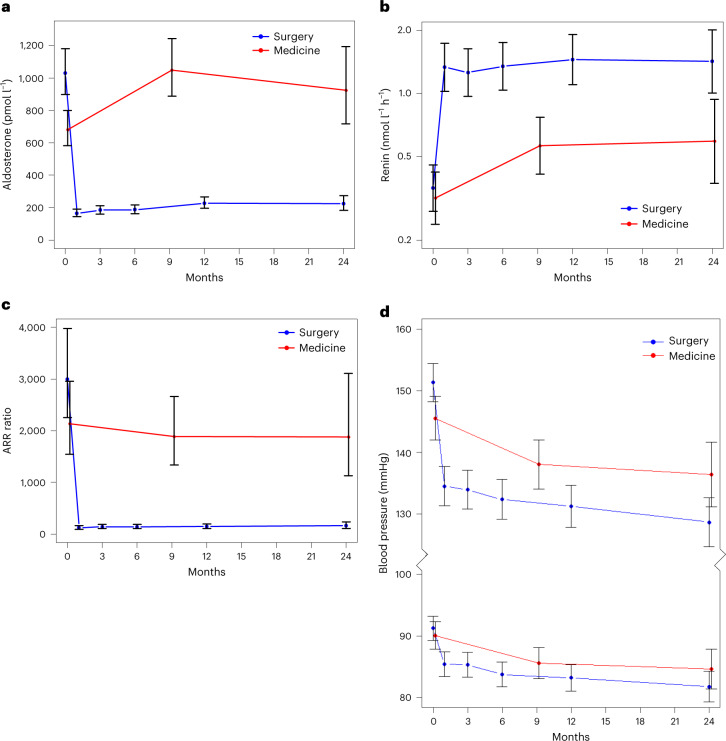
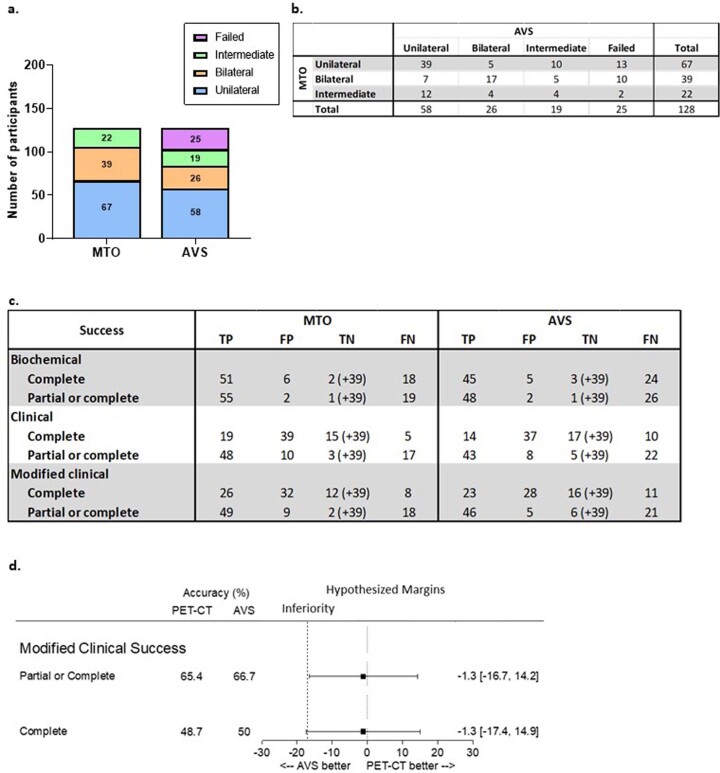
Primary aldosteronism (PA) due to a unilateral aldosterone-producing adenoma is a common cause of hypertension. This can be cured, or greatly improved, by adrenal surgery. However, the invasive nature of the standard pre-surgical investigation contributes to fewer than 1% of patients with PA being offered the chance of a cure. The primary objective of our prospective study of 143 patients with PA ( NCT02945904 ) was to compare the accuracy of a non-invasive test, [11C]metomidate positron emission tomography computed tomography (MTO) scanning, with adrenal vein sampling (AVS) in predicting the biochemical remission of PA and the resolution of hypertension after surgery. A total of 128 patients reached 6- to 9-month follow-up, with 78 (61%) treated surgically and 50 (39%) managed medically. Of the 78 patients receiving surgery, 77 achieved one or more PA surgical outcome criterion for success. The accuracies of MTO at predicting biochemical and clinical success following adrenalectomy were, respectively, 72.7 and 65.4%. For AVS, the accuracies were 63.6 and 61.5%. MTO was not significantly superior, but the differences of 9.1% (95% confidence interval = -6.5 to 24.1%) and 3.8% (95% confidence interval = -11.9 to 9.4) lay within the pre-specified -17% margin for non-inferiority (P = 0.00055 and P = 0.0077, respectively). Of 24 serious adverse events, none was considered related to either investigation and 22 were fully resolved. MTO enables non-invasive diagnosis of unilateral PA.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Non-invasive detection of a common, surgically correctable form of hypertension.Nat Med. 2023 Jan;29(1):31-32. doi: 10.1038/s41591-022-02083-9. Nat Med. 2023. PMID: 36646799 No abstract available.
