

Bariatric surgery reduces sleep apnea in obese patients with obstructive sleep apnea by increasing pharyngeal cross-sectional area during the early postoperative period
- PMID: 36646937
- PMCID: PMC10066071
- DOI: 10.1007/s00405-023-07821-4
Bariatric surgery reduces sleep apnea in obese patients with obstructive sleep apnea by increasing pharyngeal cross-sectional area during the early postoperative period
Abstract
Objective: Bariatric surgery (BS) is considered one of the most effective treatments for obese individuals with Obstructive Sleep Apnea (OSA). However, otolaryngologists have raised concerns about the structural alterations caused by BS on the upper respiratory tract, especially, on the pharyngeal cavity.
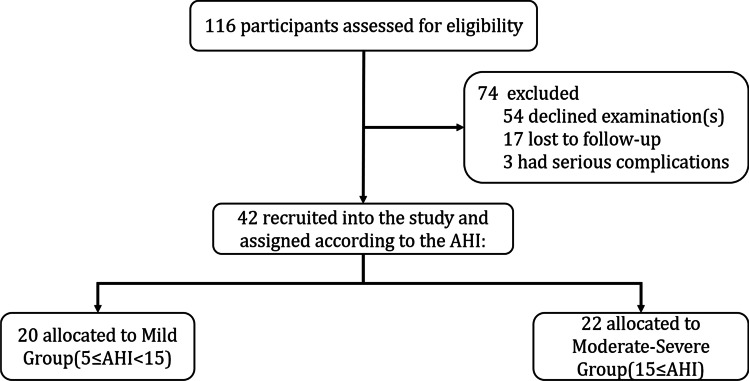
Methods: In this study, we recruited 42 individuals who underwent BS at our hospital. They were divided into two groups based on apnea-hypopnea index (AHI): mild group (5 ≤ AHI < 15) and moderate-severe group (AHI ≥ 15). The participants were followed up for 12 months and several indicators, including body mass index (BMI), polysomnography (PSG), and acoustic pharyngometry (APh), were assessed repeatedly before surgery and at 3, 6, and 12 months (m) after surgery.
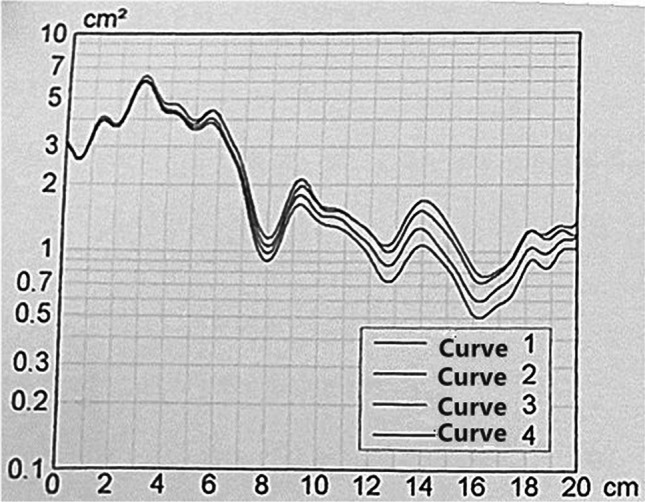
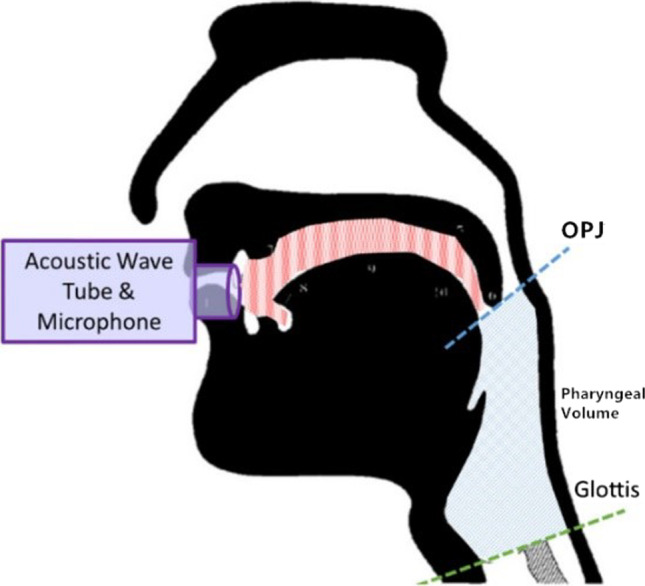
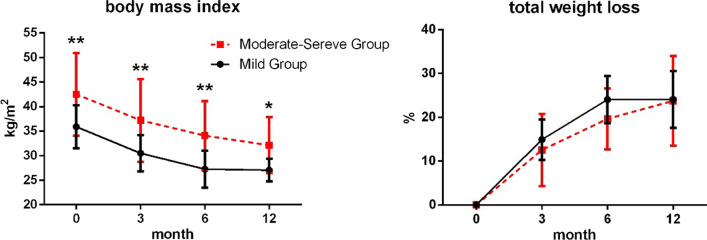
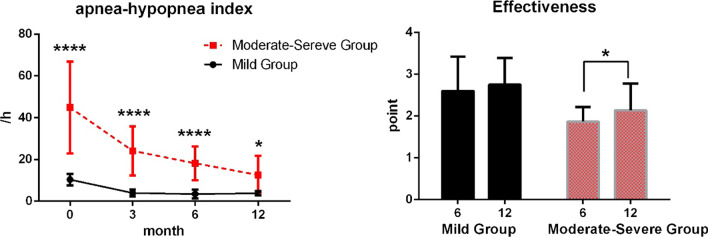
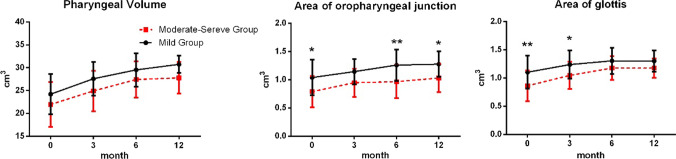
Results: Participants exhibited significant decreases in BMI (F = 128.1, P = 0.001) and total weight loss (F = 176.7, P < 0.001) after BS. The AHI value among obese patients with mild OSA decreased significantly within three months after surgery (0 day vs. 3 months, P < 0.01), and decreased significantly more than 12 months with moderate-to-severe patients (0 day vs. 3 months, 3 months vs. 6 months, 6 months vs. 12 months, P < 0.01). The therapeutic effect of OSA of the mild group was significantly better compared with that of the moderate-severe group at 6 months (mean rank = 28.13 vs. 14.21, P < 0.001) and 12 m (mean rank = 26.75 vs. 15.52, P = 0.001). The APh results revealed that the pharyngeal volume of the two groups increased significantly between 0 day and 6 months after surgery (P < 0.01). The oropharyngeal junction (OPJ) area and the glottal area were increased significantly between 0 day and 6 m after surgery (P < 0.01).
Conclusion: BS can relieve apnea and OSA symptoms among obese patients with OSA, especially in the early postoperative period. Moreover, OSA severity was closely associated with OPJ and glottal areas, rather than pharyngeal cavity volume.
Keywords: Bariatric surgery; Obstructive sleep apnea; Pharyngeal cross-sectional area.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Senaratna CV, Perret JL, Lodge CJ, Lowe AJ, Campbell BE, Matheson MC, Hamilton GS, Dharmage SC (2016) Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med Rev 34:70–81. 10.1016/j.smrv.2016.07.002 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
