

Plasma concentration and eGFR in preterm and term neonates receiving gentamicin or successive amikacin therapy
- PMID: 36647065
- PMCID: PMC9841723
- DOI: 10.1186/s12887-023-03834-4
Plasma concentration and eGFR in preterm and term neonates receiving gentamicin or successive amikacin therapy
Abstract
Background: Gentamicin and amikacin are aminoglycoside antibiotics which are renally excreted and known to be nephrotoxic. Estimate of glomerular filtration rate (eGFR) per body surface area is lower in neonates than in adults and exposure to these drugs could lead to more suppression in kidney function. The aim of this study was to determine maximum and minimum plasma concentrations (Cmax and Cmin), time to reach Cmin levels of gentamicin and amikacin, and to assess eGFR in preterm and term neonates.
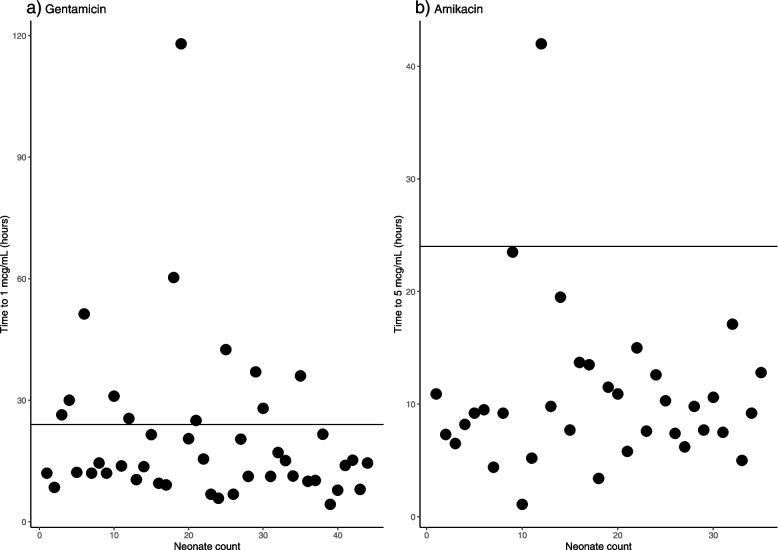
Methods: Two groups of patients were recruited, 44 neonates receiving gentamicin (5 mg/kg/24 h) and 35 neonates receiving amikacin (15 mg/kg/24 h) by slow intravenous injection. Patients on amikacin had been on gentamicin before being switched to amikacin. Two blood samples were drawn for the determination of the maximum and minimum plasma concentration. Primary outcomes were determination of Cmax, Cmin, and the time it took to clear the aminoglycoside to a plasma concentration below the toxicity threshold (gentamicin: < 1 mcg/mL; amikacin: < 5 mcg/mL.
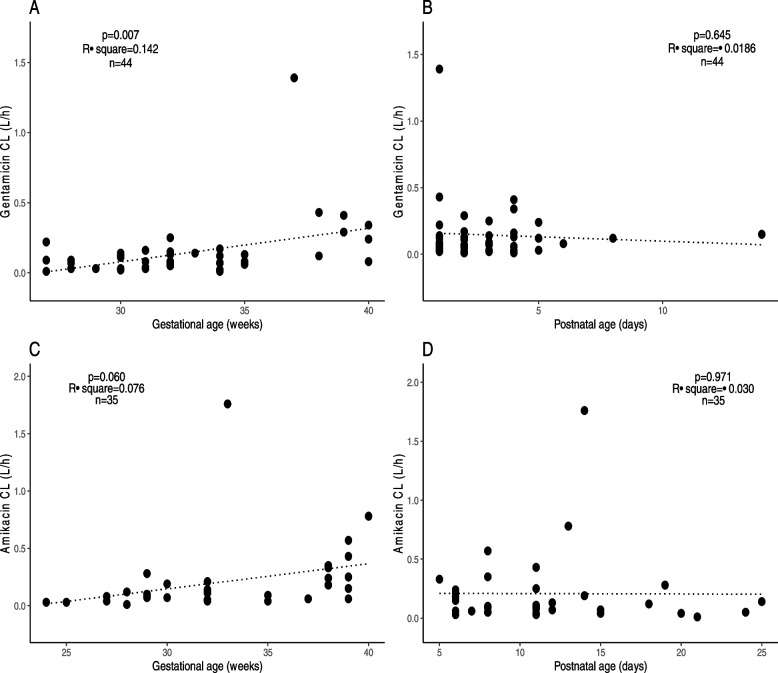
Results: Therapeutic range for Cmax of gentamicin (15-25 mcg/mL) or amikacin (30-40 mcg/mL) was achieved in only 27.3 and 2.9% of neonates, respectively. Percentage of neonates reaching plasma concentrations below the toxicity threshold within the 24-hour dosing interval was 72.7% for gentamicin and 97.1% for amikacin. Positive correlation between gentamicin clearance and postnatal age borderline statistical significance (p = 0.007), while the correlation between amikacin clearance and postnatal age was poor and not statistically significant (r2 = - 0.30, p = 0.971).
Conclusion: Although eGFR decreased significantly as a function of postnatal age in neonates receiving amikacin, the majority (91.4%) of these neonates were able to clear the drug to < 5 mcg/mL within a 24-hour dosing interval.
Keywords: Amikacin; Gentamicin; Kidney function; Neonates; Nephrotoxicity.
© 2023. The Author(s).
Conflict of interest statement
The authors have no conflicts of interest to declare that are relevant of the content of this article.
Figures

References
-
- Aminoglycosides MDC. In: Goodman & Gillman’s the pharmacological basis of therapeutics. 13. Brunton LL, Hilal-Dandal R, Knollmann BC, editors. New York: McGraw Hill; 2018. pp. 1039–1047.
-
- Thummel KE, Shen DD, Isoherranen N. Design and optimization of dosage regimens: pharmacokinetic data. In: Brunton L, Chabner B, Knollman B, editors. Goodman & Gillman’s the pharmacological basis of therapeutics. 13. New York: McGraw Hill; 2018. pp. 1325–1377.
-
- Lietman PS, Smith CR. Aminoglycoside nephrotoxicity in humans. J Infect Dis. 1983;5(Suppl 2):S284–S292.
-
- de Jager P, van Altena R. Hearing loss and nephrotoxicity in long-term aminoglycoside treatment in patients with tuberculosis. Int J Tuberc Lung Dis. 2002;6(7):622–627. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
