

Secondary Budd-Chiari syndrome occurred after adjuvant radiotherapy for perihilar cholangiocarcinoma: a case report
- PMID: 36647103
- PMCID: PMC9841655
- DOI: 10.1186/s12957-023-02890-5
Secondary Budd-Chiari syndrome occurred after adjuvant radiotherapy for perihilar cholangiocarcinoma: a case report
Abstract
Background: Budd-Chiari syndrome (BCS) is a rare vascular disorder of the liver, and acute and secondary BCS is even rarer.
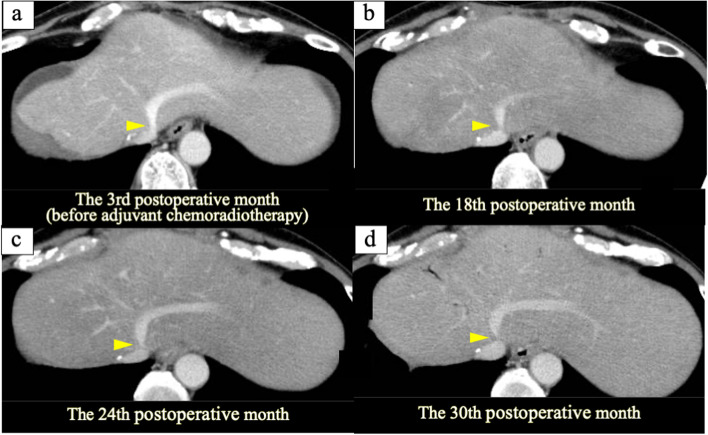
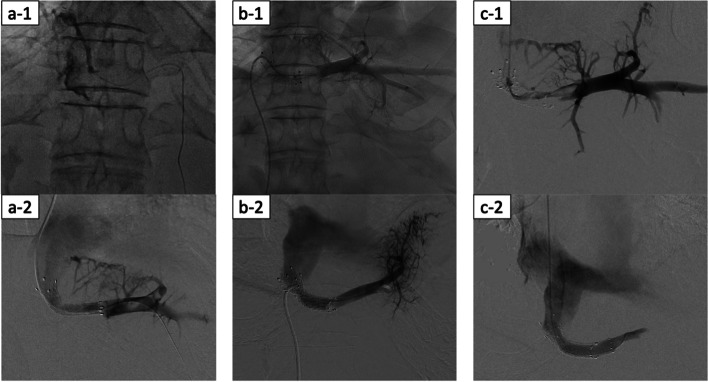
Case presentation: A 62-year-old man with perihilar cholangiocarcinoma of Bismuth type IIIa underwent right hemi-hepatectomy with caudate lobectomy and pancreatoduodenectomy. Adjuvant chemoradiotherapy was performed due to a positive hepatic ductal margin. Subsequently, the disease passed without recurrence. The patient visited for acute onset abdominal pain at the 32nd postoperative month. Multidetector-row computed tomography (MDCT) showed stenosis of the left hepatic vein (LHV) root, which was the irradiated field, and thrombotic occlusion of the LHV. The patient was diagnosed with acute BCS caused by adjuvant radiotherapy. Although anticoagulation therapy was performed, the patient complained of sudden upper abdominal pain again. MDCT showed an enlarged LHV thrombus and hepatomegaly. The patient was diagnosed with exacerbated acute BCS, and stenting for the stenotic LHV root was performed with a bare stent. Although stenting for the LHV root was very effective, restenosis occurred twice due to thrombus in the existing stent, so re-stenting was performed twice. The subsequent clinical course was acceptable without recurrence or restenosis of the LHV root as of 6 months after the last stenting using a stent graft.
Conclusion: Although no case of BCS caused by radiotherapy has yet been reported, the present case showed that late side effect of radiotherapy can cause hepatic vein stenosis and secondary BCS.
Keywords: Adjuvant radiotherapy; Budd–Chiari syndrome; Radiation-induced stenosis of the hepatic vein; Stenosis of the hepatic vein; Stenting for the hepatic vein; The side effect of radiation.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



Similar articles
-
Good Clinical Outcomes in Budd-Chiari Syndrome with Hepatic Vein Occlusion.Dig Dis Sci. 2016 Oct;61(10):3054-3060. doi: 10.1007/s10620-016-4208-0. Epub 2016 May 25. Dig Dis Sci. 2016. PMID: 27221497
-
Primary hepatic hemangioendothelioma in a patient with Budd-Chiari syndrome.BMJ Case Rep. 2017 Oct 19;2017:bcr2017221103. doi: 10.1136/bcr-2017-221103. BMJ Case Rep. 2017. PMID: 29054942 Free PMC article.
-
Treatment of Budd-Chiari syndrome by side-to-side portacaval shunt: experimental and clinical results.Ann Surg. 1978 Oct;188(4):494-512. doi: 10.1097/00000658-197810000-00007. Ann Surg. 1978. PMID: 697434 Free PMC article.
-
Budd-Chiari syndrome caused by Behçet's disease: treatment by side-to-side portacaval shunt.J Am Coll Surg. 1999 Apr;188(4):396-407. doi: 10.1016/s1072-7515(99)00012-5. J Am Coll Surg. 1999. PMID: 10195724 Review.
-
Intractable radicular and low back pain secondary inferior vena cava stenosis associated with Budd-Chiari syndrome: endovascular treatment with cava stenting: case report and review of the literature.Spine (Phila Pa 1976). 2006 May 20;31(12):E383-6. doi: 10.1097/01.brs.0000219516.54500.97. Spine (Phila Pa 1976). 2006. PMID: 16721285 Review.
Cited by
-
Adverse Events After Carbon-Ion Radiotherapy (CIRT) for Hepatocellular Carcinoma and Risk Factors for Biliary Stricture After CIRT: A Retrospective Study.Cancers (Basel). 2025 Jul 31;17(15):2542. doi: 10.3390/cancers17152542. Cancers (Basel). 2025. PMID: 40805237 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
