

Ensartinib in advanced ALK-positive non-small cell lung cancer: a multicenter, open-label, two-staged, phase 1 trial
- PMID: 36647478
- PMCID: PMC9840022
- DOI: 10.21037/jtd-22-1606
Ensartinib in advanced ALK-positive non-small cell lung cancer: a multicenter, open-label, two-staged, phase 1 trial
Abstract
Background: Ensartinib, a potent second-generation tyrosine kinase inhibitor (TKI) that targets anaplastic lymphoma kinase (ALK), MET and ROS1, was evaluated in a phase I clinical trial in patients with advanced, ALK-rearranged non-small cell lung cancer (NSCLC).
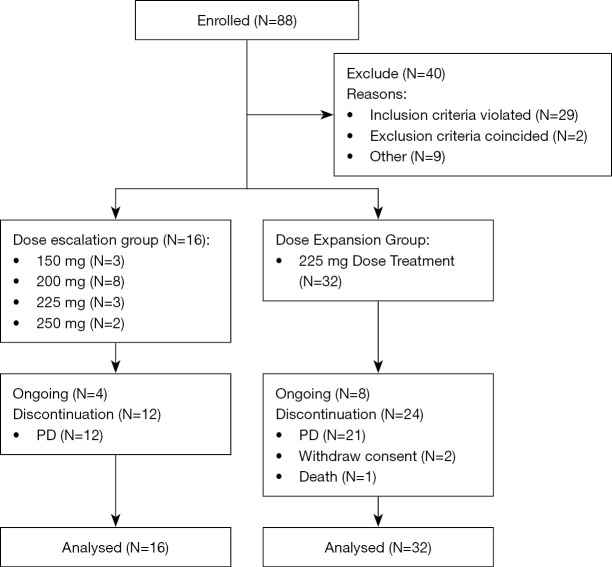
Methods: Patients with advanced, ALK or ROS1-positive NSCLC were recruited from 2 centers in China. This study consisted of dose escalation and expansion stages. Patients were treated with oral ensartinib [dosage of escalation stage was from 150, 200, 225 to 250 mg per day, expansion stage was recommended phase II dose (RP2D)] in continuous 28-day cycles. The primary objectives were safety, dose limited toxicity (DLT), maximum tolerated dose (MTD), and RP2D based on tolerability. Key secondary objectives included pharmacokinetic (PK) and anti-tumor activity.
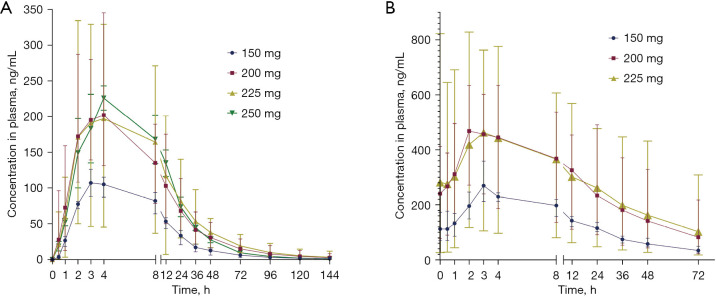
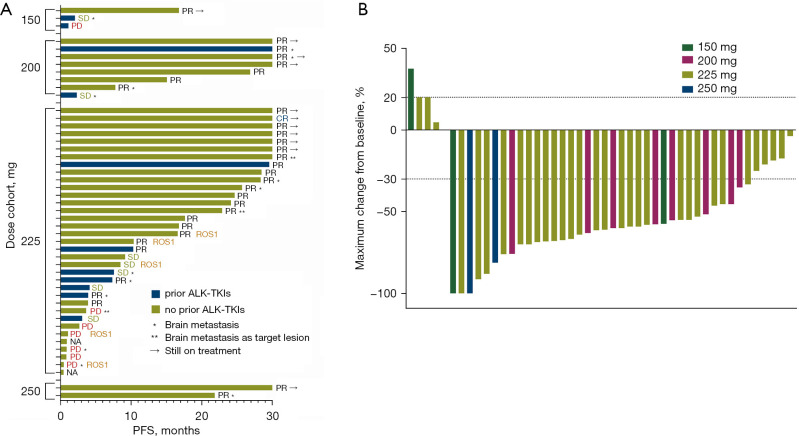
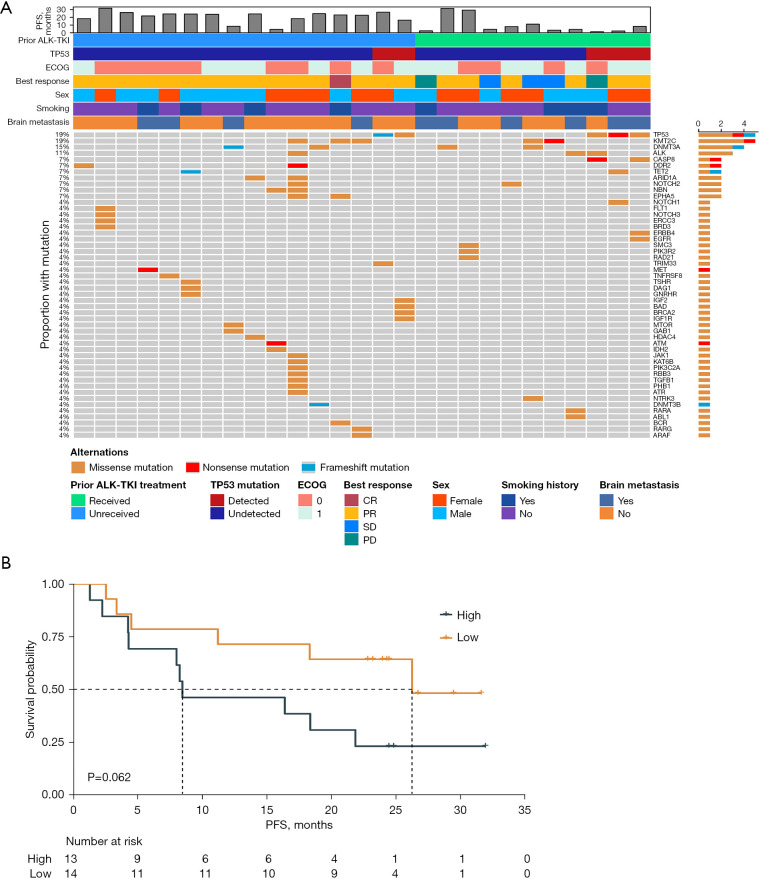
Results: Forty-eight patients were enrolled, 37 (77.1%) were ALK TKI-naïve, 11 (22.9%) patients had previously received crizotinib, ceritinib or alectinib. Ensartinib was well tolerated and common treatment-related adverse events (TRAEs) included rash (87.5%), transaminase elevation (60.4%), pruritus (45.8%) and creatinine elevation (35.4%). The top 3 grade 3-5 TRAEs were rash (14.6%), elevated alanine aminotransferase (ALT) (12.5%) and aspartate transaminase (AST) (4.2%). Two DLTs were observed in 250 mg, so MTD and RP2D was 225 mg per day. Ensartinib was moderately absorbed (median Tmax: 3.00-4.00 h) and slowly eliminated (mean T1/2: 21.0-30.2 h). The area under the curve (AUC) of ensartinib reached saturation at 200 to 225 mg and no major accumulation after daily administration. For all patients, the objective response rate (ORR) and disease control rates (DCR) were 64.6 % and 81.3%, median progression-free survival (mPFS) was 16.79 months. In subgroup analysis, the ORR and mPFS was 81.3% and 45.5%, 25.73 and 4.14 months in TKI-naïve and -treated ALK+ patients, respectively. The intra-cranial ORR and mPFS for patients with measurable brain metastases were 66.7% and 22.90 months. ALK abundance may predict the efficacy of ensartinib. Kyoto Encyclopedia of Genes and Genomes (KEGG) analysis showed specific signaling pathways enrichment in long and short progression-free survival (PFS) groups.
Conclusions: Ensartinib was well tolerated under 225 mg (MTD) and demonstrated promising anti-tumor activity in ALK+ NSCLC patients, including those with CNS metastases and those previously TKI-treated.
Trial registration: ClinicalTrials.gov NCT02959619.
Keywords: Ensartinib; anaplastic lymphoma kinase (ALK); central nervous system metastases (CNS metastases); non-small cell lung cancer (NSCLC); phase I study.
2022 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-1606/coif). SW, LZ, and HZ report funding from Betta Pharmaceuticals Co., Ltd. SW reports that the fund was managed by Zhejiang University School of Medicine Second Affiliated Hospital. LD and LC report that they are employees of Betta Pharmaceuticals Co., Ltd. SX and TW report that they are employees of Hangzhou Repugene Technology Co., Ltd. The other authors have no conflicts of interest to declare.
Figures
Similar articles
-
Conteltinib (CT-707) in patients with advanced ALK-positive non-small cell lung cancer: a multicenter, open-label, first-in-human phase 1 study.BMC Med. 2022 Nov 23;20(1):453. doi: 10.1186/s12916-022-02646-0. BMC Med. 2022. PMID: 36424628 Free PMC article. Clinical Trial.
-
Safety, Efficacy, and Biomarker Analysis of Deulorlatinib (TGRX-326) in Anaplastic Lymphoma Kinase-Positive NSCLC: A Multicenter, Open-Label, Phase 1/1b Trial.J Thorac Oncol. 2025 Jun;20(6):750-762. doi: 10.1016/j.jtho.2024.11.010. Epub 2024 Nov 15. J Thorac Oncol. 2025. PMID: 39551469 Clinical Trial.
-
Ensartinib (X-396) in ALK-Positive Non-Small Cell Lung Cancer: Results from a First-in-Human Phase I/II, Multicenter Study.Clin Cancer Res. 2018 Jun 15;24(12):2771-2779. doi: 10.1158/1078-0432.CCR-17-2398. Epub 2018 Mar 21. Clin Cancer Res. 2018. PMID: 29563138 Free PMC article. Clinical Trial.
-
Effect of alectinib versus crizotinib on progression-free survival, central nervous system efficacy and adverse events in ALK-positive non-small cell lung cancer: a systematic review and meta-analysis.Ann Palliat Med. 2020 Jul;9(4):1782-1796. doi: 10.21037/apm-19-643. Epub 2020 Jun 8. Ann Palliat Med. 2020. PMID: 32527124
-
Efficacy and Safety of First-Line Treatment Strategies for Anaplastic Lymphoma Kinase-Positive Non-Small Cell Lung Cancer: A Bayesian Network Meta-Analysis.Front Oncol. 2021 Nov 8;11:754768. doi: 10.3389/fonc.2021.754768. eCollection 2021. Front Oncol. 2021. PMID: 34820326 Free PMC article.
Cited by
-
Rutin attenuates ensartinib-induced hepatotoxicity by non-transcriptional regulation of TXNIP.Cell Biol Toxicol. 2024 May 24;40(1):38. doi: 10.1007/s10565-024-09883-4. Cell Biol Toxicol. 2024. PMID: 38789868 Free PMC article.
-
The Use of Anaplastic Lymphoma Kinase Inhibitors in Non-Small-Cell Lung Cancer Treatment-Literature Review.Biomedicines. 2024 Oct 11;12(10):2308. doi: 10.3390/biomedicines12102308. Biomedicines. 2024. PMID: 39457620 Free PMC article. Review.
-
A retrospective study of ensartinib-treated ALK-positive locally advanced or metastatic NSCLC patients in China.Lung Cancer Manag. 2023 Nov 7;12(4):LMT61. doi: 10.2217/lmt-2023-0005. eCollection 2023 Dec. Lung Cancer Manag. 2023. PMID: 38239813 Free PMC article.
-
Repotrectinib: a promising new therapy for advanced nonsmall cell lung cancer.Ann Med Surg (Lond). 2024 Nov 5;86(12):7265-7269. doi: 10.1097/MS9.0000000000002717. eCollection 2024 Dec. Ann Med Surg (Lond). 2024. PMID: 39649881 Free PMC article. Review.
-
Mechanisms of Resistance to ALK Inhibitors and Corresponding Treatment Strategies in Lung Cancer.Int J Gen Med. 2025 Apr 15;18:2151-2171. doi: 10.2147/IJGM.S512395. eCollection 2025. Int J Gen Med. 2025. PMID: 40259931 Free PMC article. Review.
References
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous