

Effect of Torsemide vs Furosemide After Discharge on All-Cause Mortality in Patients Hospitalized With Heart Failure: The TRANSFORM-HF Randomized Clinical Trial
- PMID: 36648467
- PMCID: PMC9857435
- DOI: 10.1001/jama.2022.23924
Effect of Torsemide vs Furosemide After Discharge on All-Cause Mortality in Patients Hospitalized With Heart Failure: The TRANSFORM-HF Randomized Clinical Trial
Abstract
Importance: Although furosemide is the most commonly used loop diuretic in patients with heart failure, some studies suggest a potential benefit for torsemide.
Objective: To determine whether torsemide results in decreased mortality compared with furosemide among patients hospitalized for heart failure.
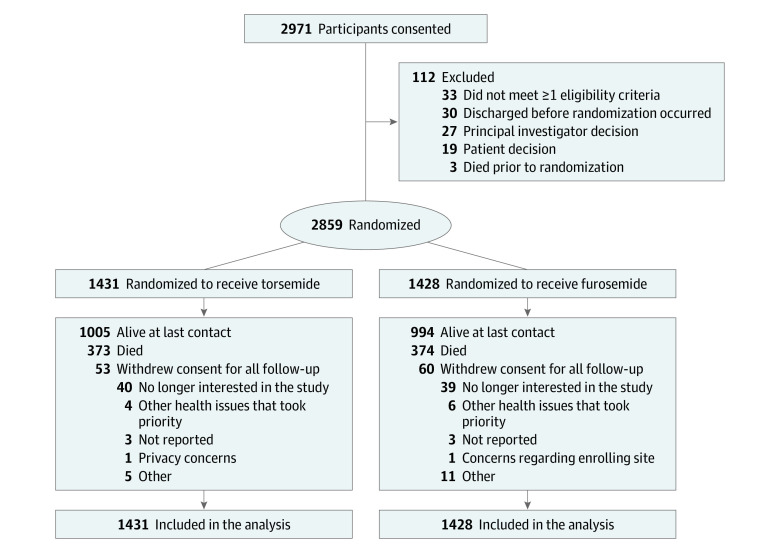
Design, setting, and participants: TRANSFORM-HF was an open-label, pragmatic randomized trial that recruited 2859 participants hospitalized with heart failure (regardless of ejection fraction) at 60 hospitals in the United States. Recruitment occurred from June 2018 through March 2022, with follow-up through 30 months for death and 12 months for hospitalizations. The final date for follow-up data collection was July 2022.
Interventions: Loop diuretic strategy of torsemide (n = 1431) or furosemide (n = 1428) with investigator-selected dosage.
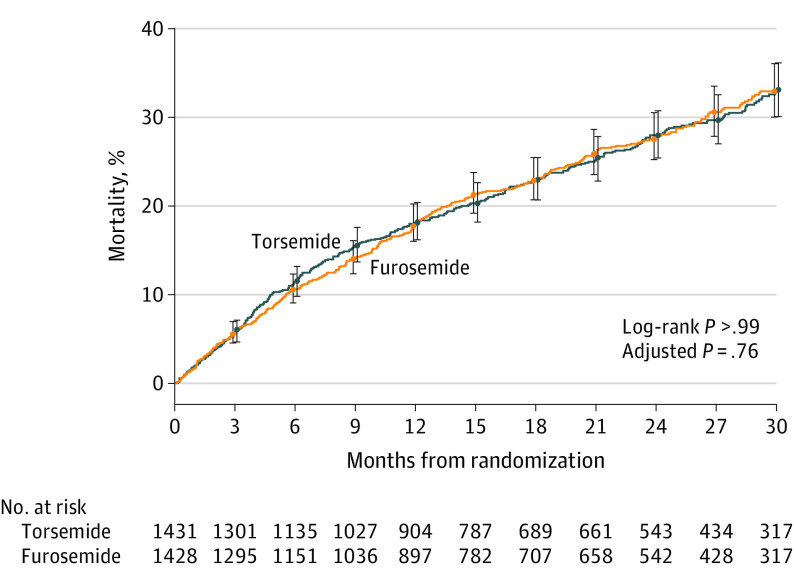
Main outcomes and measures: The primary outcome was all-cause mortality in a time-to-event analysis. There were 5 secondary outcomes with all-cause mortality or all-cause hospitalization and total hospitalizations assessed over 12 months being highest in the hierarchy. The prespecified primary hypothesis was that torsemide would reduce all-cause mortality by 20% compared with furosemide.
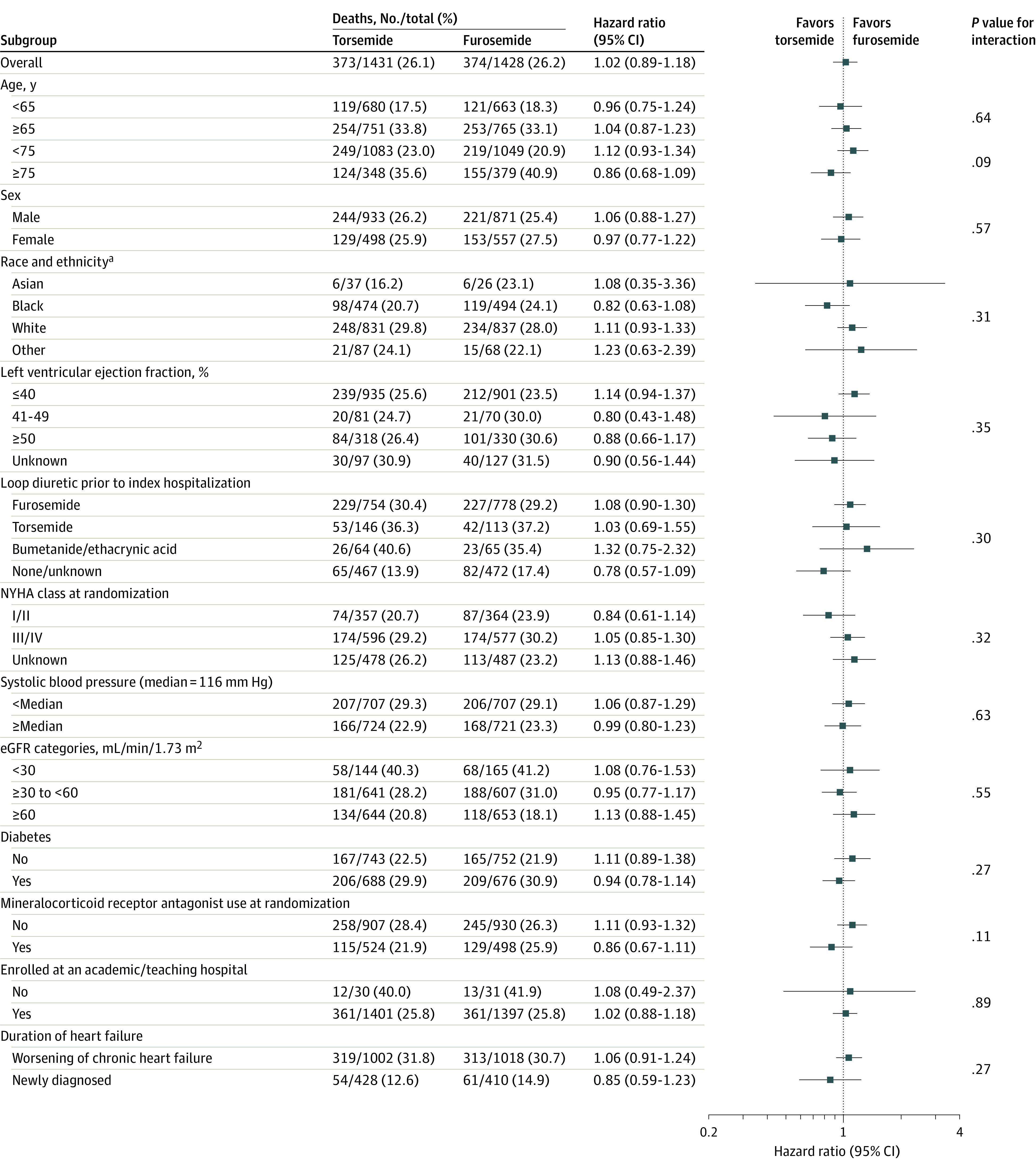
Results: TRANSFORM-HF randomized 2859 participants with a median age of 65 years (IQR, 56-75), 36.9% were women, and 33.9% were Black. Over a median follow-up of 17.4 months, a total of 113 patients (53 [3.7%] in the torsemide group and 60 [4.2%] in the furosemide group) withdrew consent from the trial prior to completion. Death occurred in 373 of 1431 patients (26.1%) in the torsemide group and 374 of 1428 patients (26.2%) in the furosemide group (hazard ratio, 1.02 [95% CI, 0.89-1.18]). Over 12 months following randomization, all-cause mortality or all-cause hospitalization occurred in 677 patients (47.3%) in the torsemide group and 704 patients (49.3%) in the furosemide group (hazard ratio, 0.92 [95% CI, 0.83-1.02]). There were 940 total hospitalizations among 536 participants in the torsemide group and 987 total hospitalizations among 577 participants in the furosemide group (rate ratio, 0.94 [95% CI, 0.84-1.07]). Results were similar across prespecified subgroups, including among patients with reduced, mildly reduced, or preserved ejection fraction.
Conclusions and relevance: Among patients discharged after hospitalization for heart failure, torsemide compared with furosemide did not result in a significant difference in all-cause mortality over 12 months. However, interpretation of these findings is limited by loss to follow-up and participant crossover and nonadherence.
Trial registration: ClinicalTrials.gov Identifier: NCT03296813.
Conflict of interest statement
Figures
Comment in
-
TRANSFORM-HF-Can We Close the Loop on Diuretics in Heart Failure?JAMA. 2023 Jan 17;329(3):211-213. doi: 10.1001/jama.2022.21692. JAMA. 2023. PMID: 36648482 No abstract available.
-
Torsemide vs Furosemide After Discharge and All-Cause Mortality in Patients With Heart Failure.JAMA. 2023 May 16;329(19):1703-1704. doi: 10.1001/jama.2023.5288. JAMA. 2023. PMID: 37191707 No abstract available.
References
-
- Tsao CW, Aday AW, Almarzooq ZI, et al. . Heart disease and stroke statistics-2022 update: a report from the American Heart Association. Circulation. 2022;145(8):e153-e639. - PubMed
-
- Braunwald E. Heart failure. JACC Heart Fail. 2013;1(1):1-20. - PubMed
-
- Faris RF, Flather M, Purcell H, Poole-Wilson PA, Coats AJ. Diuretics for heart failure. Cochrane Database Syst Rev. 2012;(2):CD003838. - PubMed
-
- Khan MS, Greene SJ, Hellkamp AS, et al. . Diuretic changes, health care resource utilization, and clinical outcomes for heart failure with reduced ejection fraction: from the Change the Management of Patients With Heart Failure Registry. Circ Heart Fail. 2021;14(11):e008351. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
