

Molnupiravir for the treatment of COVID-19 in immunocompromised participants: efficacy, safety, and virology results from the phase 3 randomized, placebo-controlled MOVe-OUT trial
- PMID: 36648627
- PMCID: PMC9844162
- DOI: 10.1007/s15010-022-01959-9
Molnupiravir for the treatment of COVID-19 in immunocompromised participants: efficacy, safety, and virology results from the phase 3 randomized, placebo-controlled MOVe-OUT trial
Abstract
Purpose: Immunocompromised patients have a potentially increased risk for progression to severe COVID-19 and prolonged replication of SARS-CoV-2. This post hoc analysis examined outcomes among immunocompromised participants in the MOVe-OUT trial.
Methods: In phase 3 of MOVe-OUT, non-hospitalized at-risk adults with mild-to-moderate COVID-19 were randomized to receive molnupiravir 800 mg or placebo twice daily for 5 days. Immunocompromised participants were identified based on prior/concomitant medications and/or medical history. All-cause hospitalization/death, adverse events, SARS-CoV-2 titers, infectivity, and RNA sequences were compared between immunocompromised participants who received molnupiravir or placebo and with non-immunocompromised participants.
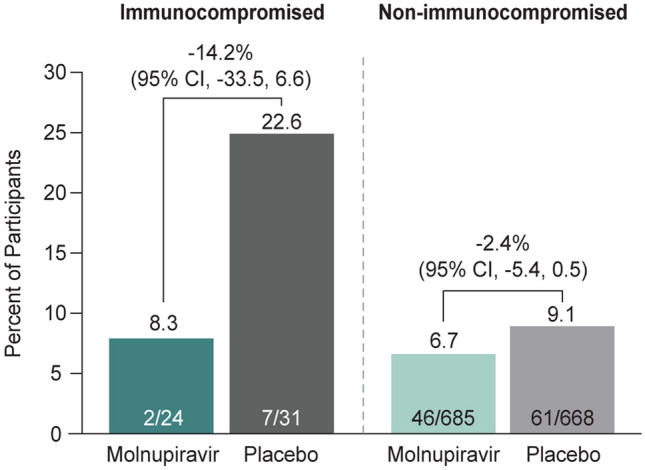
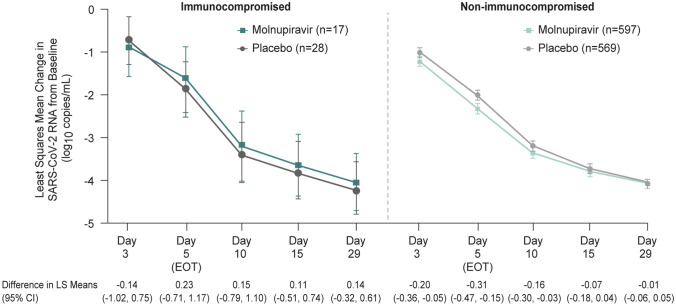
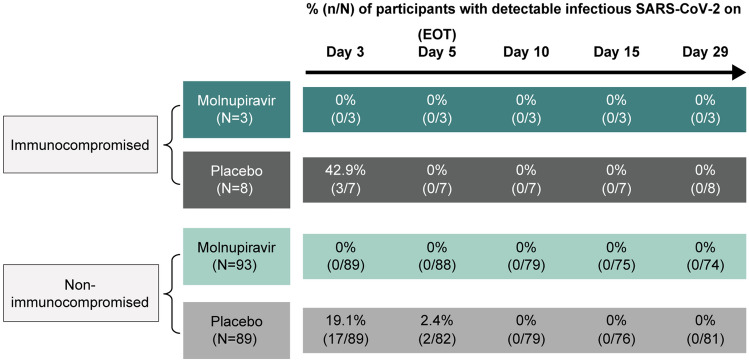
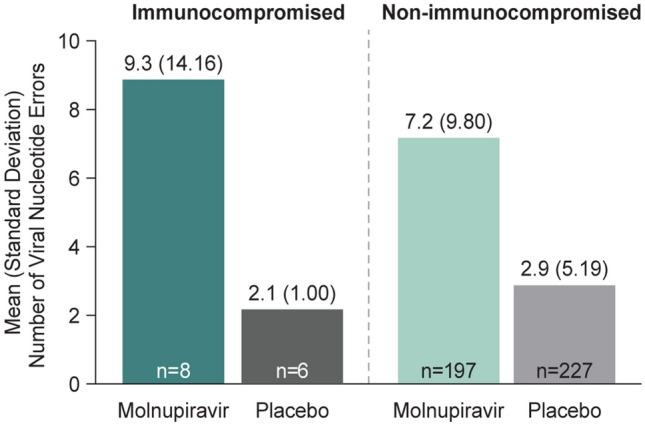
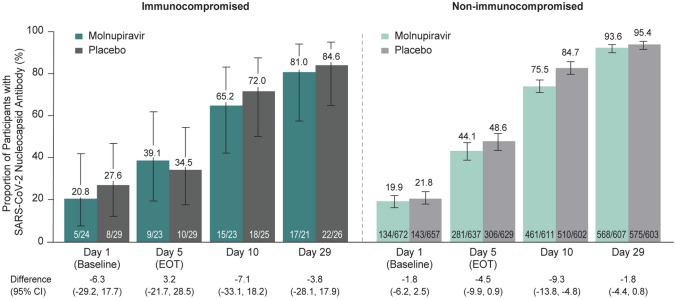
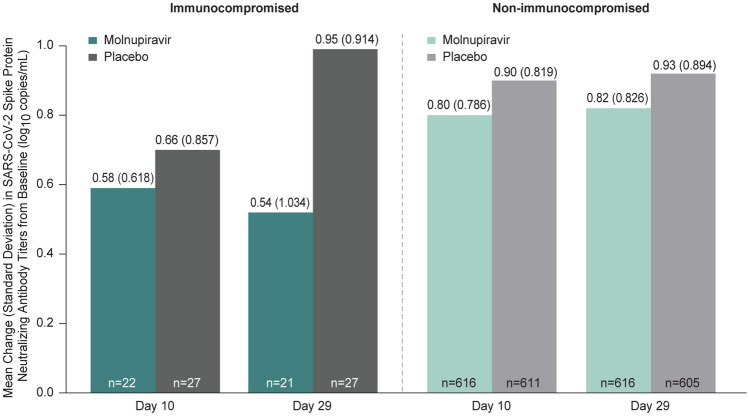
Results: Fifty-five of 1408 participants were considered immunocompromised. Compared to placebo, fewer molnupiravir-treated immunocompromised participants were hospitalized/died through Day 29 (22.6% [7/31] vs. 8.3% [2/24]), with fewer adverse events (45.2% [14/31] vs. 25.0% [6/24]). A larger mean change from baseline in SARS-CoV-2 RNA was observed with molnupiravir compared to placebo in non-immunocompromised participants (least squares mean [LSM] difference Day 5: - 0.31, 95% confidence interval [CI] - 0.47 to - 0.15), while the mean change was comparable between treatment groups in immunocompromised participants (LSM difference Day 5: 0.23, 95% CI - 0.71 to 1.17). Molnupiravir treatment was associated with increased clearance of infectious virus. Increased errors in viral nucleotide sequences in post-baseline samples compared to placebo support molnupiravir's mechanism of action and were not associated with observation of novel treatment-emergent amino acid substitutions in immunocompromised participants.
Conclusion: Although the study population was small, these data suggest that molnupiravir treatment for mild-to-moderate COVID-19 in non-hospitalized immunocompromised adults is efficacious and safe and quickly reduces infectious SARS-CoV-2.
Gov registration number: NCT04575597.
Keywords: COVID-19; Immunocompromised; Molnupiravir; Treatment; Virology.
© 2023. Merck & Co., Inc., Rahway, NJ, USA and its affiliates.
Conflict of interest statement
Matthew G. Johnson, Julie M. Strizki, Michelle L. Brown, Hong Wan (at the time of study), Hala H. Shamsuddin, Angela Williams-Diaz, Jiejun Du (at the time of study), Jay A. Grobler, Amanda Paschke, and Carisa De Anda are employees of Merck & Co., Inc., Rahway, NJ, USA. Moti Ramgopal: Consulting fees: Gilead, Merck, ViiV, Janssen; Honoraria: Gilead, ViiV, Janssen. Diana F. Florescu: Grants: Merck, Regeneron, Astellas, Novavax, Bavarian Nordic, Takeda, SymBio, NobelPharma, AlloVir. Consulting fees: Takeda and Merck; Data Safety Monitoring Board/Advisory Board: Medpace. Pierre Delobel: Travel grants: BMS, Gilead, MSD, and Janssen in the last 5 years; Society: HAS/ANRS-MIE/CNS: French recommendations for treatment and prevention of HIV, hepatitis, and STIs; Scientific Committee: ANRS-MIE (CSS13). Ilsiyar Khaertynova: Nothing to disclose. José F. Flores: Nothing to disclose. Leon F. Fouche: Nothing to disclose. Shan-Chwen Chang: Nothing to disclose.
Figures
Comment in
-
Molnupiravir efficacy among immunocompromised patients with COVID-19: no proof of concept.Infection. 2023 Oct;51(5):1593-1595. doi: 10.1007/s15010-023-02027-6. Epub 2023 Apr 1. Infection. 2023. PMID: 37004695 Free PMC article. No abstract available.
References
-
- Kim L, Garg S, O'Halloran A, et al. Risk factors for intensive care unit admission and in-hospital mortality among hospitalized adults identified through the US Coronavirus Disease 2019 (COVID-19)-Associated Hospitalization Surveillance Network (COVID-NET) Clin Infect Dis. 2021;72(9):e206–e214. doi: 10.1093/cid/ciaa1012. - DOI - PMC - PubMed
-
- Team TNCPERE. The epidemiological characteristics of an outbreak of 2019 Novel Coronavirus Diseases (COVID-19) - China, 2020. China CDC Wkly. 2020;2(8):113–22, https://www.ncbi.nlm.nih.gov/pubmed/34594836. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
