

Efficacy and safety of bimekizumab in axial spondyloarthritis: results of two parallel phase 3 randomised controlled trials
- PMID: 36649967
- PMCID: PMC10086273
- DOI: 10.1136/ard-2022-223595
Efficacy and safety of bimekizumab in axial spondyloarthritis: results of two parallel phase 3 randomised controlled trials
Erratum in
-
Correction: Efficacy and safety of bimekizumab in axial spondyloarthritis: results of two parallel phase 3 randomised controlled trials.Ann Rheum Dis. 2023 Sep;82(9):e213. doi: 10.1136/ard-2022-223595corr1. Epub 2023 Jul 3. Ann Rheum Dis. 2023. PMID: 37402489 Free PMC article. No abstract available.
Abstract
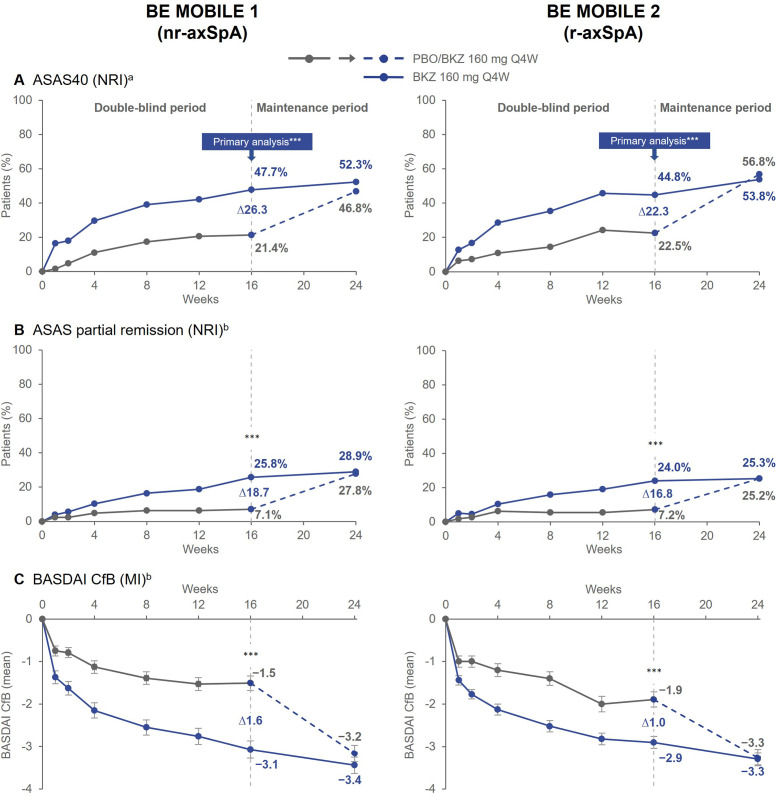
Objectives: Axial spondyloarthritis (axSpA) is a complex disease with diverse manifestations, for which new treatment options are warranted. BE MOBILE 1 (non-radiographic (nr)-axSpA) and BE MOBILE 2 (radiographic axSpA (r-axSpA)) are double-blind, phase 3 trials designed to evaluate efficacy and safety of bimekizumab, a novel dual interleukin (IL)-17A and IL-17F inhibitor, across the axSpA spectrum.
Methods: In parallel 52-week trials, patients with active disease were randomised 1:1 (nr-axSpA) or 2:1 (r-axSpA) to bimekizumab 160 mg every 4 weeks:placebo. From week 16, all patients received bimekizumab 160 mg every 4 weeks. Primary (Assessment of SpondyloArthritis international Society ≥40% improvement (ASAS40)) and secondary endpoints were assessed at week 16. Here, efficacy and treatment-emergent adverse events (TEAEs) are reported up to week 24.
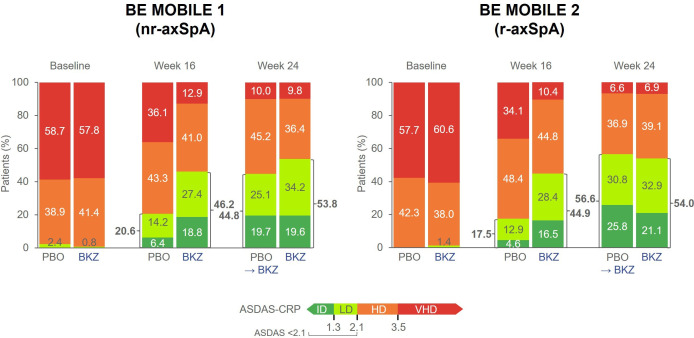
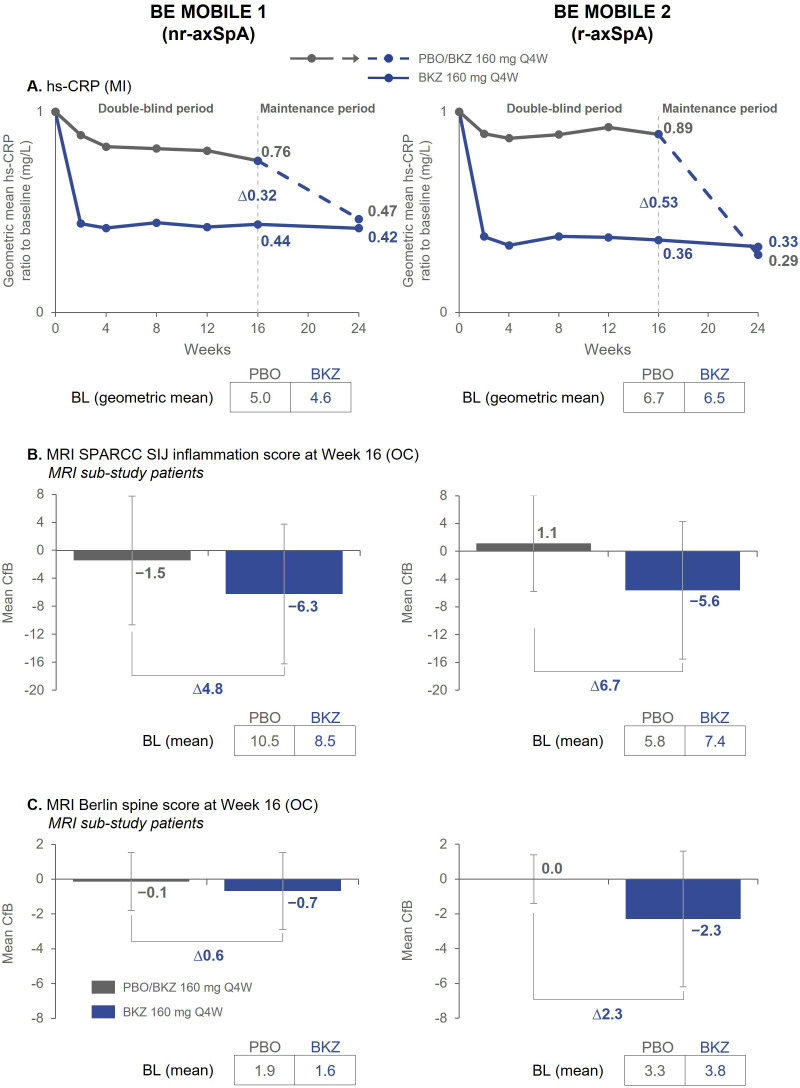
Results: 254 patients with nr-axSpA and 332 with r-axSpA were randomised. At week 16, primary (ASAS40, nr-axSpA: 47.7% bimekizumab vs 21.4% placebo; r-axSpA: 44.8% vs 22.5%; p<0.001) and all ranked secondary endpoints were met in both trials. ASAS40 responses were similar across TNFi-naïve and TNFi-inadequate responder patients. Improvements were observed in Ankylosing Spondylitis Disease Activity Score (ASDAS) states and objective measures of inflammation, including high-sensitivity C-reactive protein (hs-CRP) and MRI of the sacroiliac joints and spine. Most frequent TEAEs with bimekizumab (>3%) included nasopharyngitis, upper respiratory tract infection, pharyngitis, diarrhoea, headache and oral candidiasis. More fungal infections (all localised) were observed with bimekizumab vs placebo; no major adverse cardiovascular events (MACE) or active tuberculosis were reported. Incidence of uveitis and adjudicated inflammatory bowel disease was low.
Conclusions: Dual inhibition of IL-17A and IL-17F with bimekizumab resulted in significant and rapid improvements in efficacy outcomes vs placebo and was well tolerated in patients with nr-axSpA and r-axSpA.
Keywords: Autoimmune Diseases; Biological Therapy; Cytokines; Inflammation; Spondylitis, Ankylosing.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: DvdH: Consulting fees from AbbVie, Bayer, BMS, Cyxone, Eisai, Galapagos, Gilead, GSK, Janssen, Lilly, Novartis, Pfizer, UCB Pharma, and is the director of Imaging Rheumatology BV; AD: Speaker for Janssen, Novartis, and Pfizer; consultant of AbbVie, Amgen, Aurinia, BMS, Celgene, Eli Lilly, GSK, Janssen, MoonLake, Novartis, Pfizer, and UCB Pharma; grant/research support from AbbVie, Eli Lilly, GSK, Novartis, Pfizer, and UCB Pharma; XB: Speaker for AbbVie, BMS, Chugai, Eli Lilly, Galapagos, Gilead, MSD, Novartis, Pfizer, and UCB Pharma; paid instructor for AbbVie, BMS, Chugai, Eli Lilly, Galapagos, Gilead, MSD, Novartis, Pfizer, and UCB Pharma; consultant for AbbVie, BMS, Chugai, Eli Lilly, Galapagos, Gilead, MSD, Novartis, Pfizer, and UCB Pharma; MAB: Grant/research support from UCB; Consultant for Clementia, Grey Wolf Therapeutics, Incyte, Ipsen, Pfizer, Regeneron, and Xinthera; Speaker for Novartis; HD: Speaker for BMS, Chugai, Eli Lilly, GSK, MSD, Novartis, Pfizer, UCB Pharma; MD: Consultant for AbbVie, Eli Lilly, Novartis, Merck, Pfizer, and UCB Pharma; Grant/research support from: AbbVie, Eli Lilly, Novartis, Pfizer, and UCB Pharma; DE: Consultancy and speaker fees from AbbVie, Eli Lilly, Galapagos, Novartis and UCB Pharma; KG: Consultant of AbbVie, Eli Lilly, Novartis, and UCB Pharma; grant/research support from AbbVie, Gilead, Eli Lilly, Novartis, and UCB Pharma; speakers bureau from AbbVie, Eli Lilly, Novartis, UCB Pharma; LSG: Consulting fees from AbbVie, Eli Lilly, Gilead, Janssen, MoonLake, Novartis, Pfizer, and UCB Pharma; grant/research support from Novartis, Pfizer and UCB Pharma; NH: Consulting fees from AbbVie, Eli Lilly, Janssen, Novartis and UCB Pharma; MM: Consultancy fees from AbbVie, BMS, Eli Lilly, Novartis, Pfizer and UCB Pharma, and research grants from AbbVie, BMS and UCB Pharma; WPM: Honoraria/consulting fees from AbbVie, Boehringer-Ingelheim, Celgene, Eli Lilly, Galapagos, Janssen, Novartis, Pfizer and UCB Pharma; research grants from AbbVie, Pfizer; educational grants from AbbVie, Janssen, Novartis and Pfizer; Chief Medical Officer for CARE Arthritis; DP: Speaker for AbbVie, BMS, Eli Lilly, MSD, Novartis, Pfizer, and UCB Pharma; Consultant for AbbVie, Biocad, Eli Lilly, Gilead, GSK, MSD, Novartis, Pfizer, Samsung Bioepis, and UCB Pharma; Grant/research support from: AbbVie, MSD, Novartis, and Pfizer; MR: Speakers bureau from AbbVie, BMS, Boehringer Ingelheim, Chugai, Eli Lilly, Janssen, Novartis, Pfizer, UCB Pharma; consultant of AbbVie, Eli Lilly, Novartis, UCB Pharma; TT: Consultancy fees: AbbVie, Eli Lilly, Gilead, Novartis, and Pfizer; Speaker fees: AbbVie, Astellas, BMS, Eisai, Eli Lilly, Janssen, Kyowa Kirin, Mitsubishi-Tanabe, Novartis, and Pfizer; FVdB: Consultancy fees from AbbVie, Amgen, Eli Lilly, Galapagos, Janssen, Merck, Novartis, Pfizer and UCB Pharma; Speakers bureau fees from AbbVie, BMS, Celgene, Janssen, Merck, Novartis, Pfizer and UCB Pharma; HX: Speaker for AbbVie, Janssen, Novartis, Pfizer, and UCB Pharma; Consultant for AbbVie, Beigene, BioMap, IASO, Pfizer, and UCB Pharma; Clinical investigator for Peking-Tsinghua Center for Life Sciences; AM, UM, MO, CF, TV, AME, JSS: Employees of UCB Pharma.
Figures
Comment in
-
Bimekizumab effective across the axSpA spectrum.Nat Rev Rheumatol. 2023 Mar;19(3):127. doi: 10.1038/s41584-023-00927-3. Nat Rev Rheumatol. 2023. PMID: 36755118 No abstract available.
References
-
- Boel A, Molto A, van der Heijde D, et al. Do patients with axial spondyloarthritis with radiographic sacroiliitis fulfil both the modified New York criteria and the ASAS axial spondyloarthritis criteria? Results from eight cohorts. Ann Rheum Dis 2019;78:1545–9. 10.1136/annrheumdis-2019-215707 - DOI - PubMed
-
- Boel A, López-Medina C, van der Heijde DMFM, et al. Age at onset in axial spondyloarthritis around the world: data from the Assessment in SpondyloArthritis international Society peripheral involvement in spondyloarthritis study. Rheumatology 2022;61:1468–75. 10.1093/rheumatology/keab544 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
