

Nucleic acid drug vectors for diagnosis and treatment of brain diseases
- PMID: 36650130
- PMCID: PMC9844208
- DOI: 10.1038/s41392-022-01298-z
Nucleic acid drug vectors for diagnosis and treatment of brain diseases
Abstract
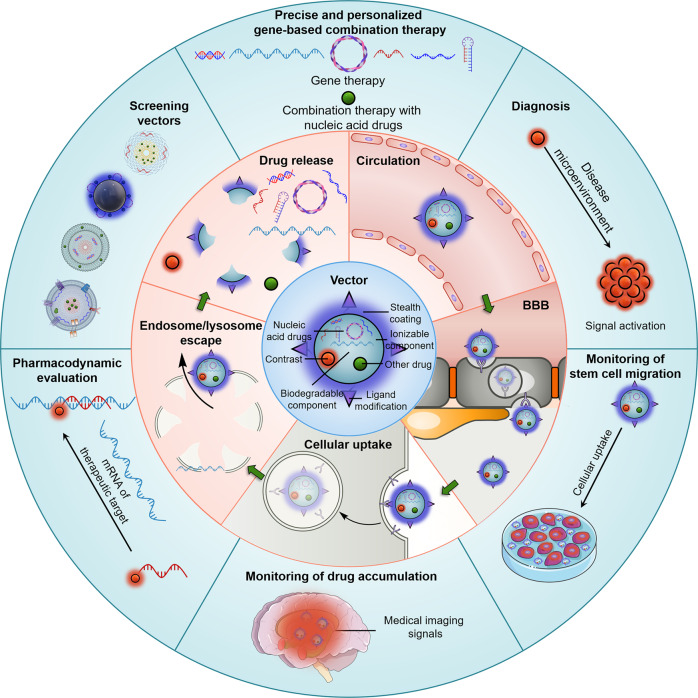
Nucleic acid drugs have the advantages of rich target selection, simple in design, good and enduring effect. They have been demonstrated to have irreplaceable superiority in brain disease treatment, while vectors are a decisive factor in therapeutic efficacy. Strict physiological barriers, such as degradation and clearance in circulation, blood-brain barrier, cellular uptake, endosome/lysosome barriers, release, obstruct the delivery of nucleic acid drugs to the brain by the vectors. Nucleic acid drugs against a single target are inefficient in treating brain diseases of complex pathogenesis. Differences between individual patients lead to severe uncertainties in brain disease treatment with nucleic acid drugs. In this Review, we briefly summarize the classification of nucleic acid drugs. Next, we discuss physiological barriers during drug delivery and universal coping strategies and introduce the application methods of these universal strategies to nucleic acid drug vectors. Subsequently, we explore nucleic acid drug-based multidrug regimens for the combination treatment of brain diseases and the construction of the corresponding vectors. In the following, we address the feasibility of patient stratification and personalized therapy through diagnostic information from medical imaging and the manner of introducing contrast agents into vectors. Finally, we take a perspective on the future feasibility and remaining challenges of vector-based integrated diagnosis and gene therapy for brain diseases.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures






References
-
- Li Y, et al. Strategies and materials of “SMART” non-viral vectors: overcoming the barriers for brain gene therapy. Nano Today. 2020;35:101006. doi: 10.1016/j.nantod.2020.101006. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
