

Comparing the accuracy of ultrasound-based measurements of the cervical vagus nerve
- PMID: 36650212
- PMCID: PMC9845339
- DOI: 10.1038/s41598-023-27894-9
Comparing the accuracy of ultrasound-based measurements of the cervical vagus nerve
Abstract
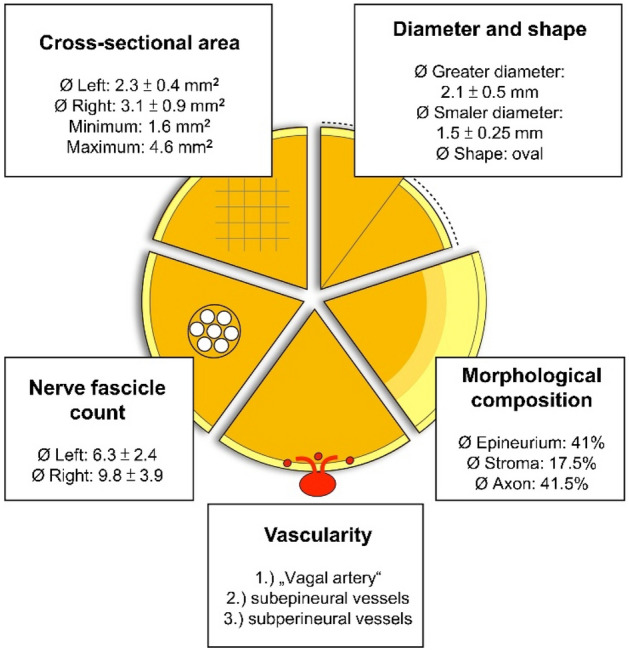
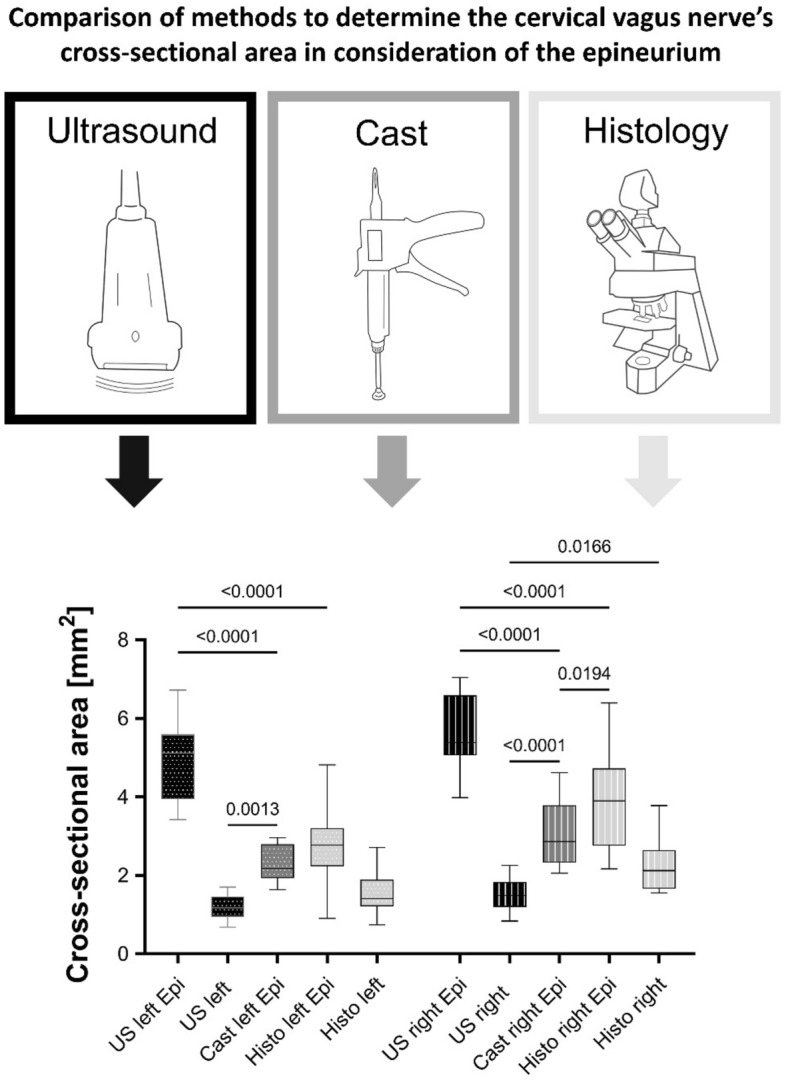
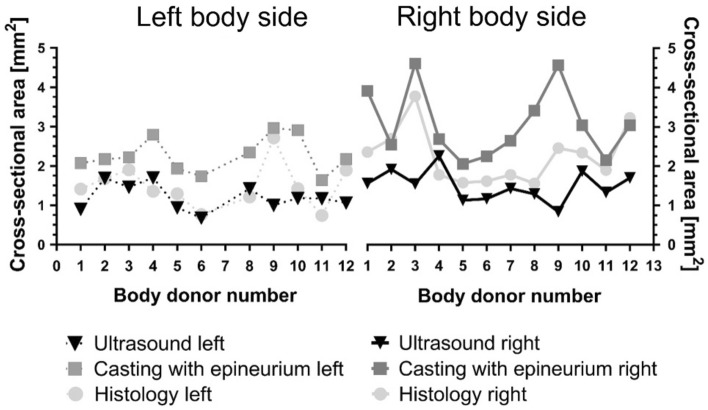
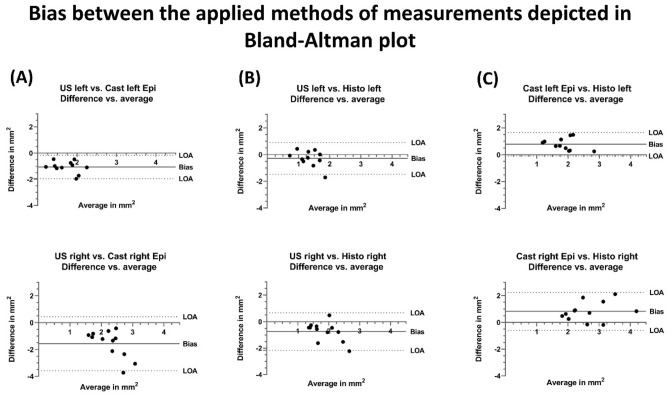
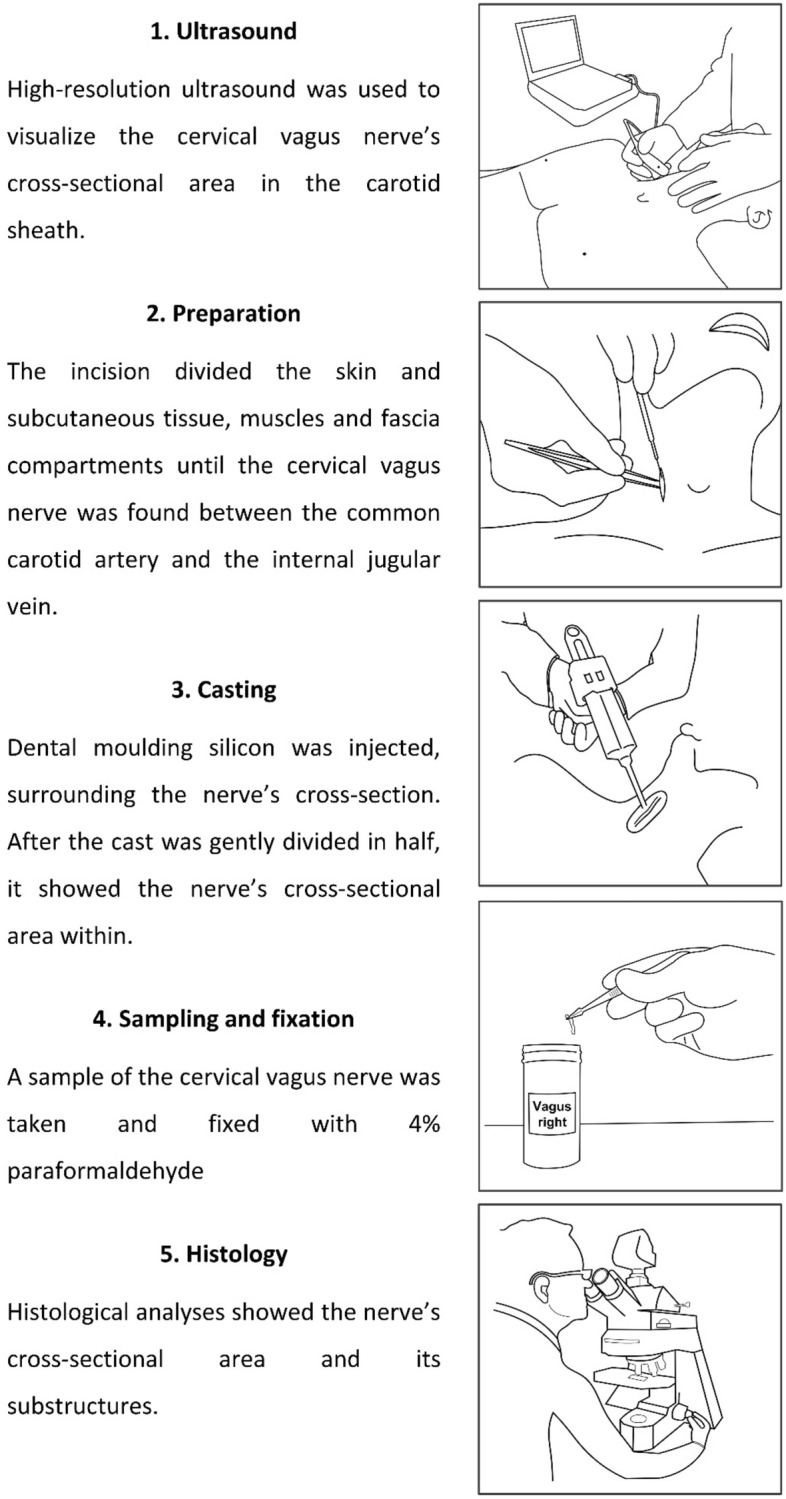
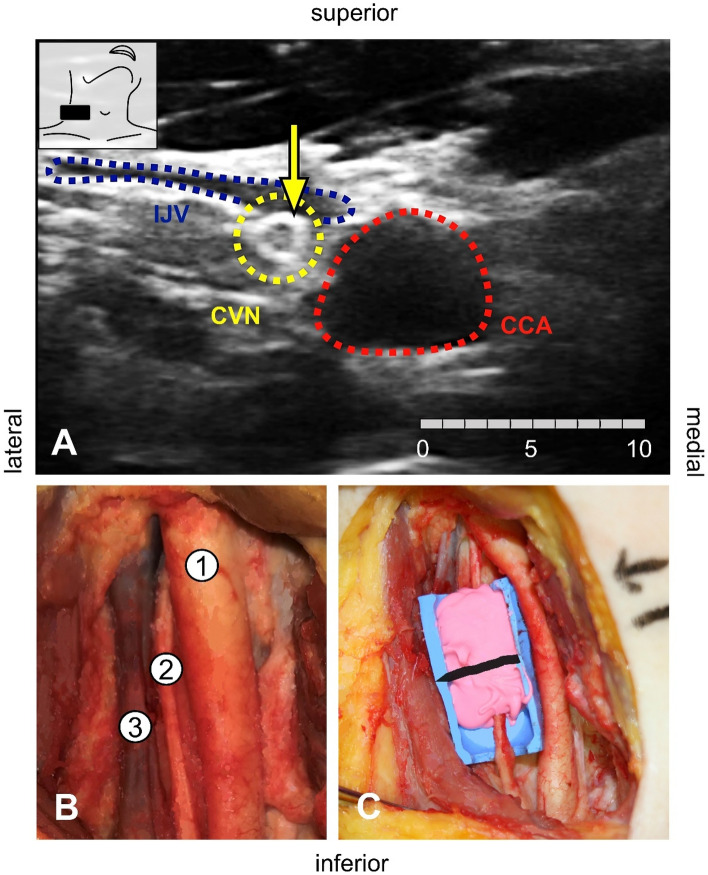
Vagus nerve stimulation (VNS) has become a promising therapy especially for drug resistant epilepsy and other pathologies. Side effects or missing therapeutic success are observed due to cuff electrodes that are too narrow or too wide. Preoperative high-resolution ultrasound is used to evaluate the size of the cervical vagus nerve (CVN) to estimate the size of cuff electrodes for VNS. It remains unclear how precise ultrasound reflects the CVN dimensions, which has been the objective of this study. CVN cross-sections and diameters were investigated in 23 sides from 12 bodies, using ultrasound, histology, and CVN casting in situ as a reference. Morphometric data were obtained including fascicle count and nerve composition in histology. CVN yielded significant side-, age-, and BMI-related differences. CVN cross-sections were smaller in ultrasound when compared to casting and histology (1.5 ± 0.4 vs. 3.1 ± 0.9 vs. 2.3 ± 0.7 mm2). With the given setting in ultrasound, CVN cross-sections were consistently underestimated when compared to casting. Ultrasound-based cross-section measurements are related to a biased estimation of CVN size. A factor to correct for method related differences may help to adjust for accurate cuff electrode sizes for patient needs and to reduce undesired effects and potentially material consumption.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Hirsch M, Reinacher P, Schulze-Bonhage A. Vagusnervstimulation in der Behandlung von Epilepsiepatienten. Akt. Neurol. 2016;43:501–510. doi: 10.1055/s-0042-116022. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
