

Effect of apneic oxygenation with intubation to reduce severe desaturation and adverse tracheal intubation-associated events in critically ill children
- PMID: 36650568
- PMCID: PMC9847056
- DOI: 10.1186/s13054-023-04304-0
Effect of apneic oxygenation with intubation to reduce severe desaturation and adverse tracheal intubation-associated events in critically ill children
Abstract
Background: Determine if apneic oxygenation (AO) delivered via nasal cannula during the apneic phase of tracheal intubation (TI), reduces adverse TI-associated events (TIAEs) in children.
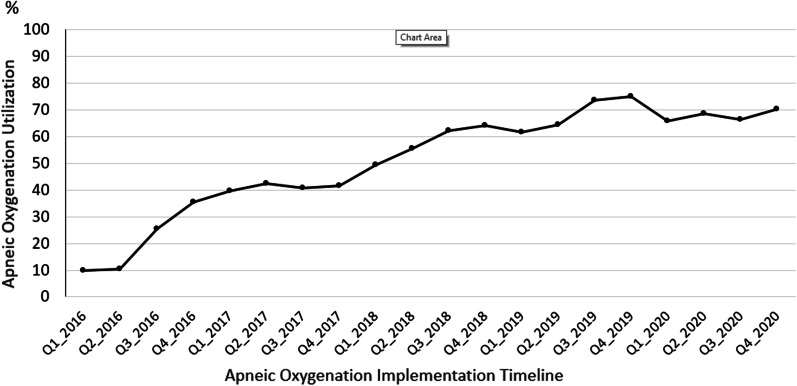
Methods: AO was implemented across 14 pediatric intensive care units as a quality improvement intervention during 2016-2020. Implementation consisted of an intubation safety checklist, leadership endorsement, local champion, and data feedback to frontline clinicians. Standardized oxygen flow via nasal cannula for AO was as follows: 5 L/min for infants (< 1 year), 10 L/min for young children (1-7 years), and 15 L/min for older children (≥ 8 years). Outcomes were the occurrence of adverse TIAEs (primary) and hypoxemia (SpO2 < 80%, secondary).
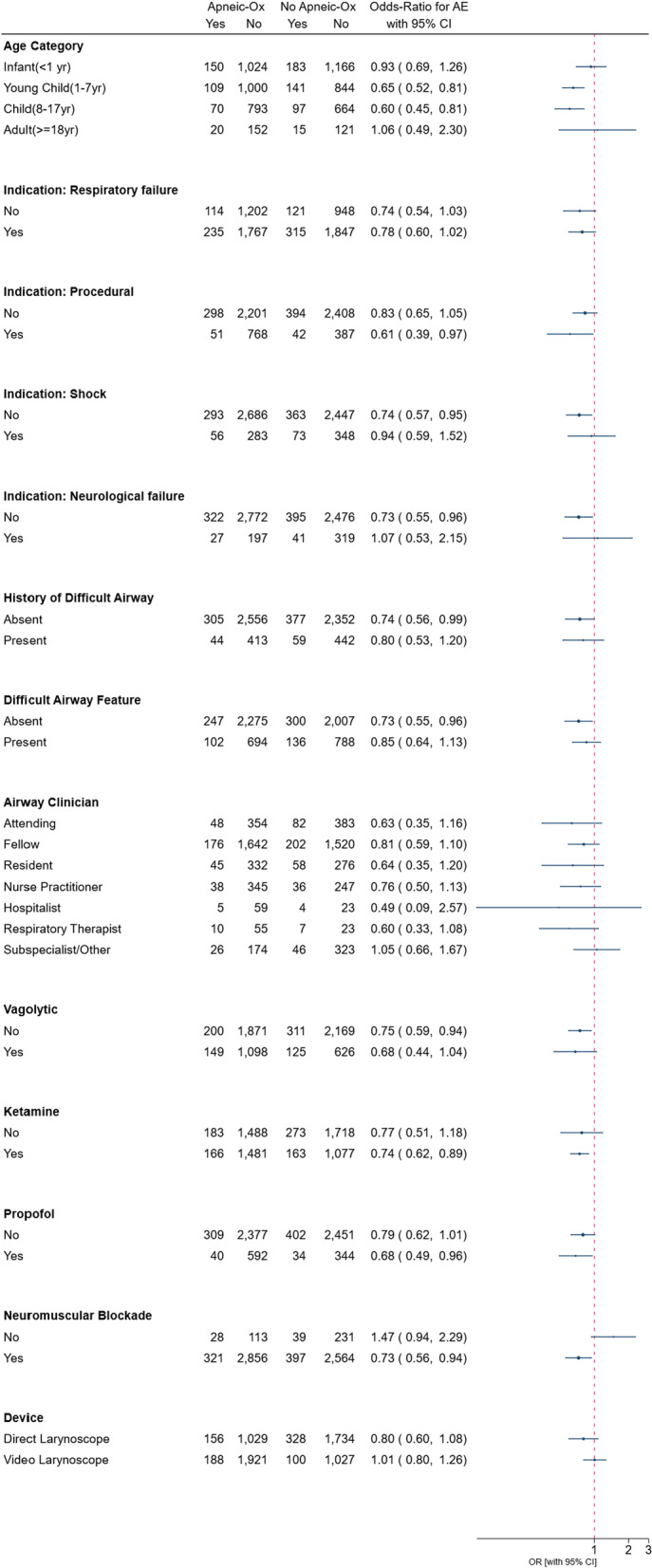
Results: Of 6549 TIs during the study period, 2554 (39.0%) occurred during the pre-implementation phase and 3995 (61.0%) during post-implementation phase. AO utilization increased from 23 to 68%, p < 0.001. AO was utilized less often when intubating infants, those with a primary cardiac diagnosis or difficult airway features, and patient intubated due to respiratory or neurological failure or shock. Conversely, AO was used more often in TIs done for procedures and those assisted by video laryngoscopy. AO utilization was associated with a lower incidence of adverse TIAEs (AO 10.5% vs. without AO 13.5%, p < 0.001), aOR 0.75 (95% CI 0.58-0.98, p = 0.03) after adjusting for site clustering (primary analysis). However, after further adjusting for patient and provider characteristics (secondary analysis), AO utilization was not independently associated with the occurrence of adverse TIAEs: aOR 0.90, 95% CI 0.72-1.12, p = 0.33 and the occurrence of hypoxemia was not different: AO 14.2% versus without AO 15.2%, p = 0.43.
Conclusion: While AO use was associated with a lower occurrence of adverse TIAEs in children who required TI in the pediatric ICU after accounting for site-level clustering, this result may be explained by differences in patient, provider, and practice factors. Trial Registration Trial not registered.
Keywords: Airway; Apneic oxygenation; Hypoxemia; Pediatrics; Tracheal intubation.
© 2023. The Author(s).
Conflict of interest statement
Mrs. Napolitano, Dr. Shults, Dr. Nadkarni, and Dr. Nishisaki received funding from AHRQ R18HS024511 for this work. Mrs. Napolitano had research and consulting relationships with Drager, Timpel, Philips/Respironics, Actuated Medical, and VERO-Biotech. Dr. Polikoff has a consulting relationship with Novavax. No other authors have conflicts of interest to declare.
Figures
References
-
- Kleinman ME, de Caen AR, Chameides L, Atkins DL, Berg RA, Berg MD, Bhanji F, Biarent D, Bingham R, Coovadia AH, Hazinski MF, Hickey RW, Nadkarni VM, Reis AG, Rodriguez-Nunez A, Tibballs J, Zaritsky AL, Zideman D, Pediatric Basic and Advanced Life Support Chapter Collaborators Part 10: pediatric basic and advanced life support: 2010 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2010;122(16 Suppl 2):S466–515. - PMC - PubMed
-
- Kleinman ME, Chameides L, Schexnayder SM, Samson RA, Hazinski MF, Atkins DL, Berg MD, de Caen AR, Fink EL, Freid EB, Hickey RW, Marino BS, Nadkarni VM, Proctor LT, Qureshi FA, Sartorelli K, Topjian A, van der Jagt EW, Zaritsky AL. Part 14: pediatric advanced life support: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010;122(18 Suppl 3):S876–908. - PubMed
-
- Nishisaki A, Turner DA, Brown CA, III, Walls RM, Nadkarni V, For the National Emergency Airway Registry for Children (NEAR4KIDS) and Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network A National Emergency Airway Registry for Children (NEAR4KIDS) landscape of tracheal intubation in 15 pediatric intensive care units. Crit Care Med. 2013;41(3):874–85. doi: 10.1097/CCM.0b013e3182746736. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
