

Emerging precision neoadjuvant systemic therapy for patients with resectable non-small cell lung cancer: current status and perspectives
- PMID: 36650586
- PMCID: PMC9847175
- DOI: 10.1186/s40364-022-00444-7
Emerging precision neoadjuvant systemic therapy for patients with resectable non-small cell lung cancer: current status and perspectives
Abstract
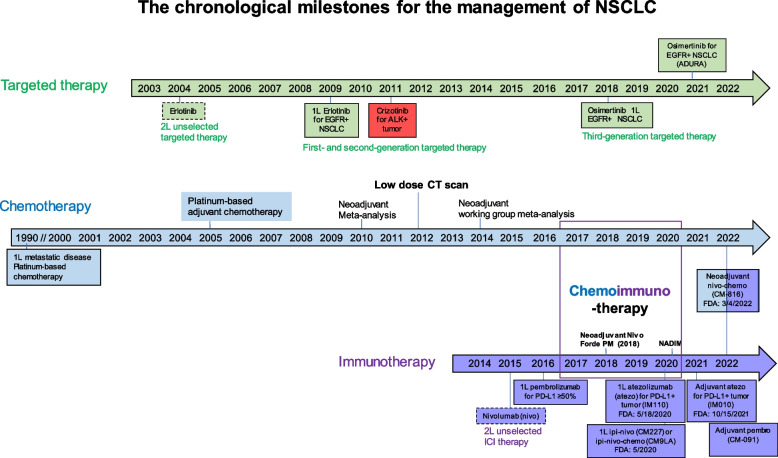
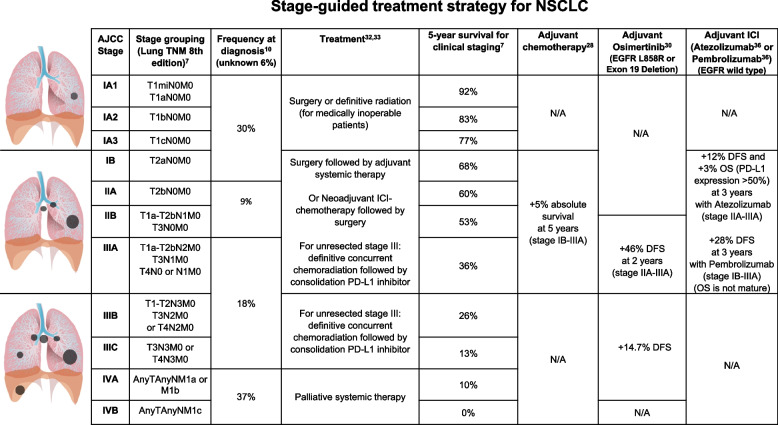
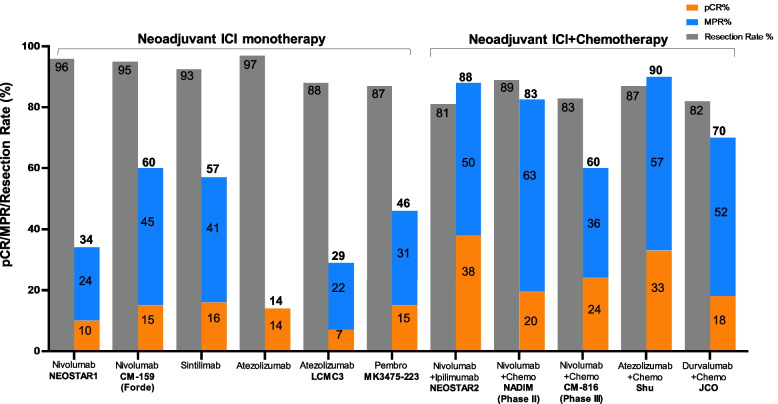
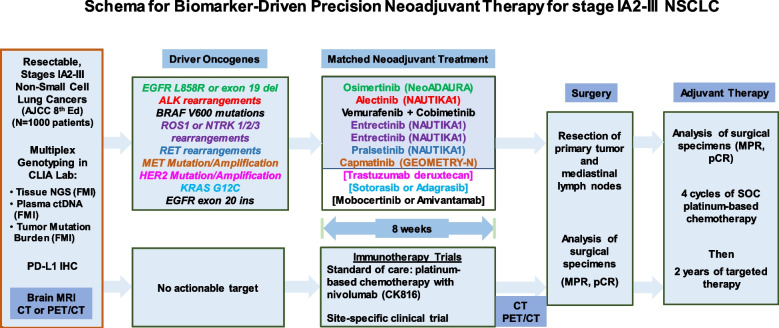
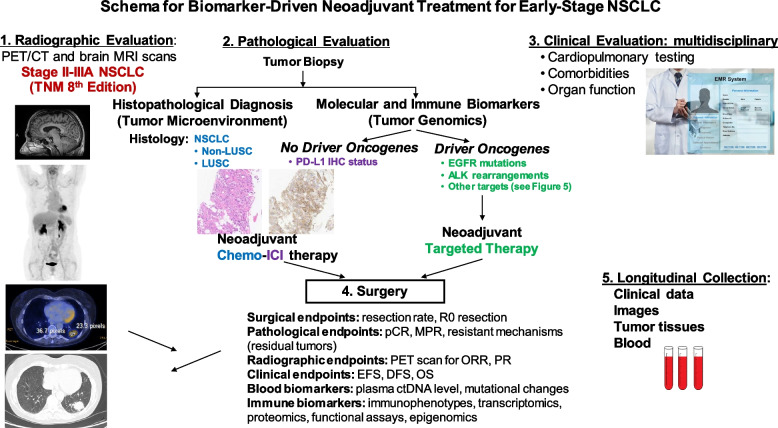
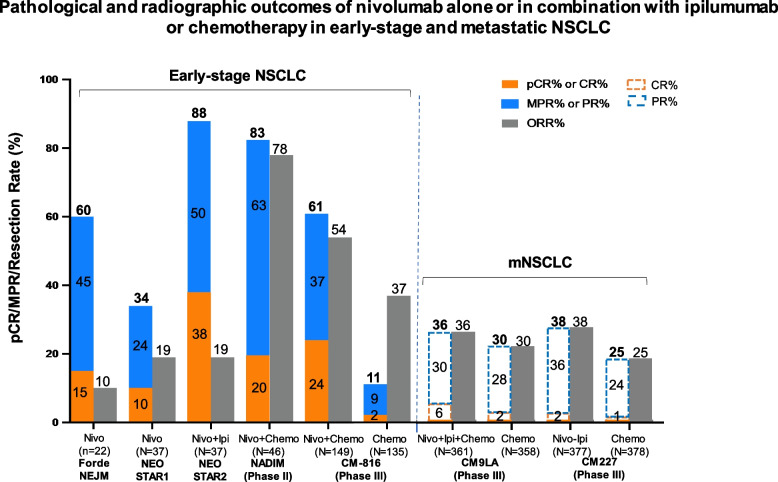
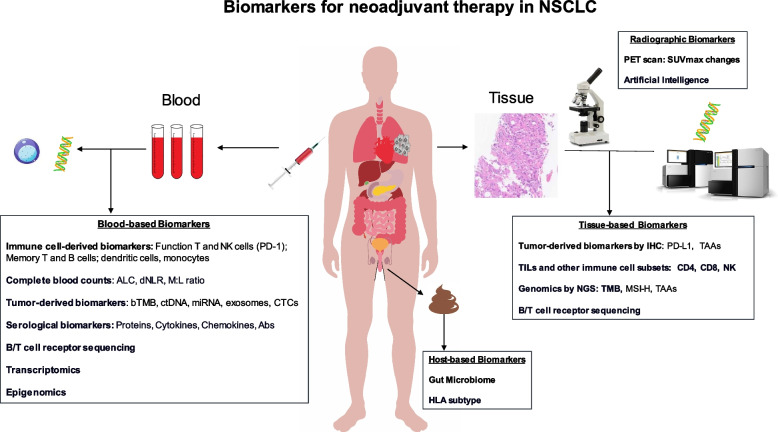
Over the past decade, targeted therapy for oncogene-driven NSCLC and immune checkpoint inhibitors for non-oncogene-driven NSCLC, respectively, have greatly improved the survival and quality of life for patients with unresectable NSCLC. Increasingly, these biomarker-guided systemic therapies given before or after surgery have been used in patients with early-stage NSCLC. In March 2022, the US FDA granted the approval of neoadjuvant nivolumab and chemotherapy for patients with stage IB-IIIA NSCLC. Several phase II/III trials are evaluating the clinical efficacy of various neoadjuvant immune checkpoint inhibitor combinations for non-oncogene-driven NSCLC and neoadjuvant molecular targeted therapies for oncogene-driven NSCLC, respectively. However, clinical application of precision neoadjuvant treatment requires a paradigm shift in the biomarker testing and multidisciplinary collaboration at the diagnosis of early-stage NSCLC. In this comprehensive review, we summarize the current diagnosis and treatment landscape, recent advances, new challenges in biomarker testing and endpoint selections, practical considerations for a timely multidisciplinary collaboration at diagnosis, and perspectives in emerging neoadjuvant precision systemic therapy for patients with resectable, early-stage NSCLC. These biomarker-guided neoadjuvant therapies hold the promise to improve surgical and pathological outcomes, reduce systemic recurrences, guide postoperative therapy, and improve cure rates in patients with resectable NSCLC.
Keywords: Immune checkpoint inhibitor (ICI); NSCLC; Neoadjuvant; Precision oncology; Resectable; Systemic therapy; Targeted therapy.
© 2022. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
