

Electric impedance tomography-guided PEEP titration reduces mechanical power in ARDS: a randomized crossover pilot trial
- PMID: 36650593
- PMCID: PMC9843117
- DOI: 10.1186/s13054-023-04315-x
Electric impedance tomography-guided PEEP titration reduces mechanical power in ARDS: a randomized crossover pilot trial
Abstract
Background: In patients with acute respiratory distress syndrome undergoing mechanical ventilation, positive end-expiratory pressure (PEEP) can lead to recruitment or overdistension. Current strategies utilized for PEEP titration do not permit the distinction. Electric impedance tomography (EIT) detects and quantifies the presence of both collapse and overdistension. We investigated whether using EIT-guided PEEP titration leads to decreased mechanical power compared to high-PEEP/FiO2 tables.
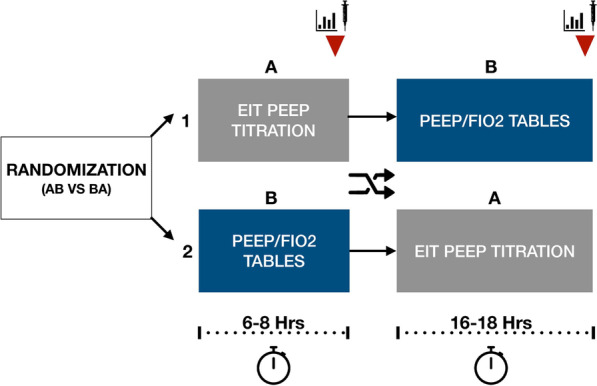
Methods: A single-center, randomized crossover pilot trial comparing EIT-guided PEEP selection versus PEEP selection using the High-PEEP/FiO2 table in patients with moderate-severe acute respiratory distress syndrome. The primary outcome was the change in mechanical power after each PEEP selection strategy. Secondary outcomes included changes in the 4 × driving pressure + respiratory rate (4 ΔP, + RR index) index, driving pressure, plateau pressure, PaO2/FiO2 ratio, and static compliance.
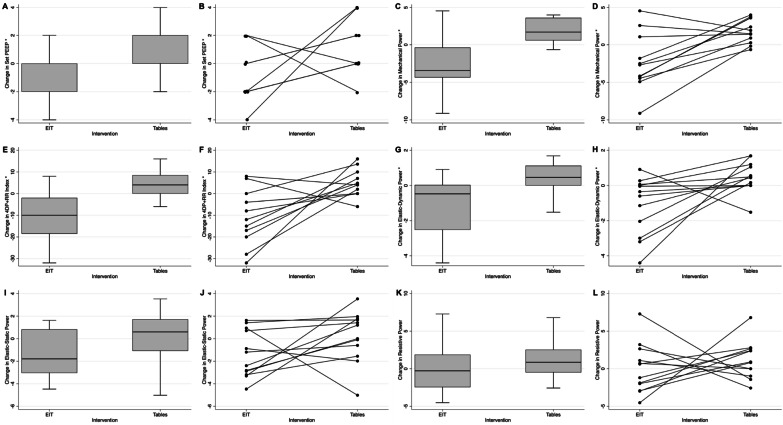
Results: EIT was consistently associated with a decrease in mechanical power compared to PEEP/FiO2 tables (mean difference - 4.36 J/min, 95% CI - 6.7, - 1.95, p = 0.002) and led to lower values in the 4ΔP + RR index (- 11.42 J/min, 95% CI - 19.01, - 3.82, p = 0.007) mainly driven by a decrease in the elastic-dynamic power (- 1.61 J/min, - 2.99, - 0.22, p = 0.027). The elastic-static and resistive powers were unchanged. Similarly, EIT led to a statistically significant change in set PEEP (- 2 cmH2O, p = 0.046), driving pressure, (- 2.92 cmH2O, p = 0.003), peak pressure (- 6.25 cmH2O, p = 0.003), plateau pressure (- 4.53 cmH2O, p = 0.006), and static respiratory system compliance (+ 7.93 ml/cmH2O, p = 0.008).
Conclusions: In patients with moderate-severe acute respiratory distress syndrome, EIT-guided PEEP titration reduces mechanical power mainly through a reduction in elastic-dynamic power. Trial registration This trial was prospectively registered on Clinicaltrials.gov (NCT03793842) on January 4th, 2019.
Keywords: Acute lung injury; Electrical impedance tomography; Mechanical ventilators; Respiratory distress syndrome; Ventilator-induced lung injury.
© 2023. The Author(s).
Conflict of interest statement
EM was supported by Grant Number T32 HL 007749 (Multidisciplinary Training Program in Lung Disease) from the National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. AW reports speaking fees from Drager and author fees from Jones and Bartlett Learning, unrelated to this work. WWL reports personal fees from Konica Minolta and Continuing Education Alliance. PC is a consultant for Breas Medical US and performs Medicolegal Expert witness work. HP reported receiving grants from the US Department of Veterans Affairs outside the submitted work, serving on the Surviving Sepsis Campaign Guidelines Panel, and serving as physician lead for a Michigan statewide sepsis collaborative. RH serves on the advisory board for Merck, Boehringer Ingelheim. Consultant for LungPacer and NOTA-Laboratories has textbook royalties from Springer Website and UpToDate. Grants: CHEST Foundation, NHLBI PETAL Network Medicolegal Expert witness work. Dräger loaned equipment (PulmoVista® 500) to RH for research purposes; no monetary funds were provided.
Figures
References
-
- Dianti J, Tisminetzky M, Ferreyro BL, et al. Association of positive end-expiratory pressure and lung recruitment selection strategies with mortality in acute respiratory distress syndrome: a systematic review and network meta-analysis. Am J Respir Crit Care Med. 2022;205(11):1300–1310. doi: 10.1164/rccm.202108-1972OC. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
