

Persistent SARS-CoV-2 infection in patients seemingly recovered from COVID-19
- PMID: 36651103
- PMCID: PMC10107739
- DOI: 10.1002/path.6035
Persistent SARS-CoV-2 infection in patients seemingly recovered from COVID-19
Abstract
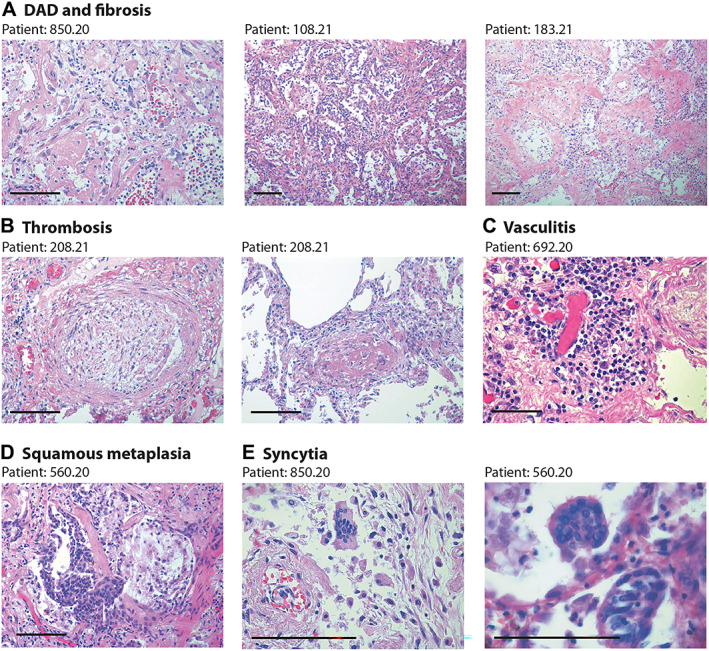
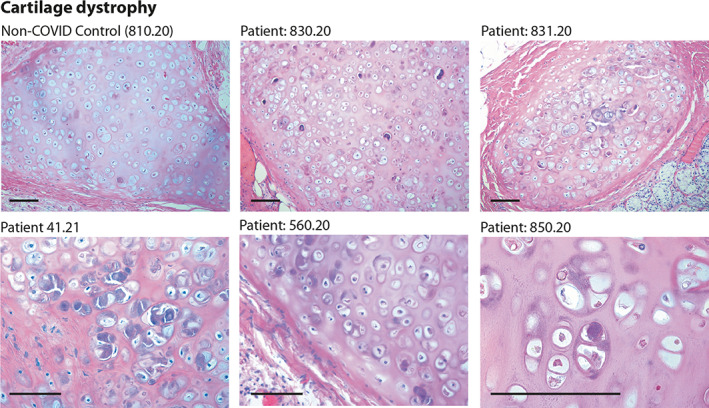
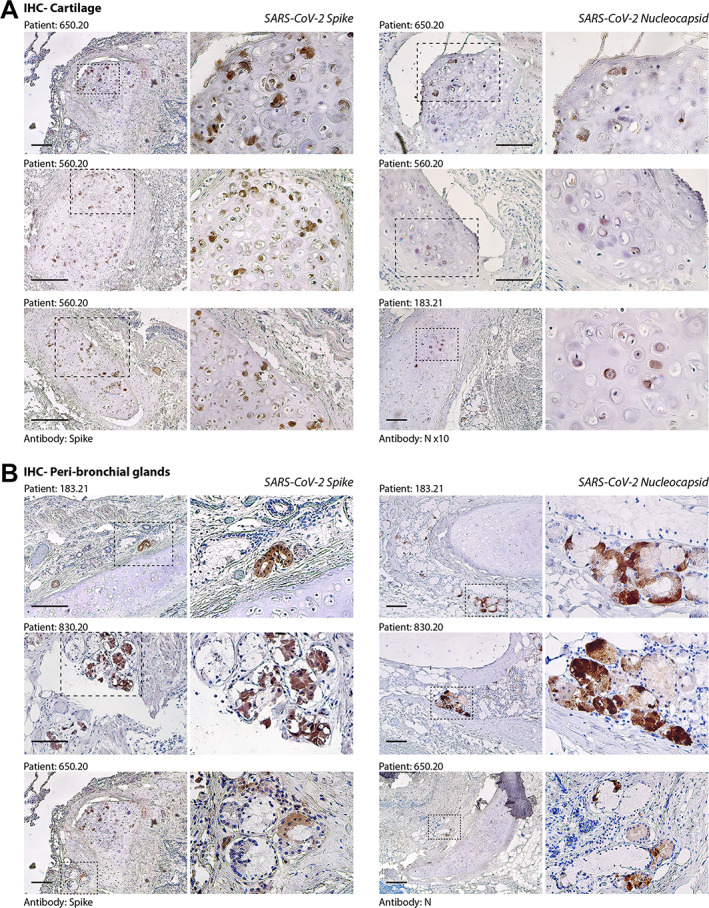
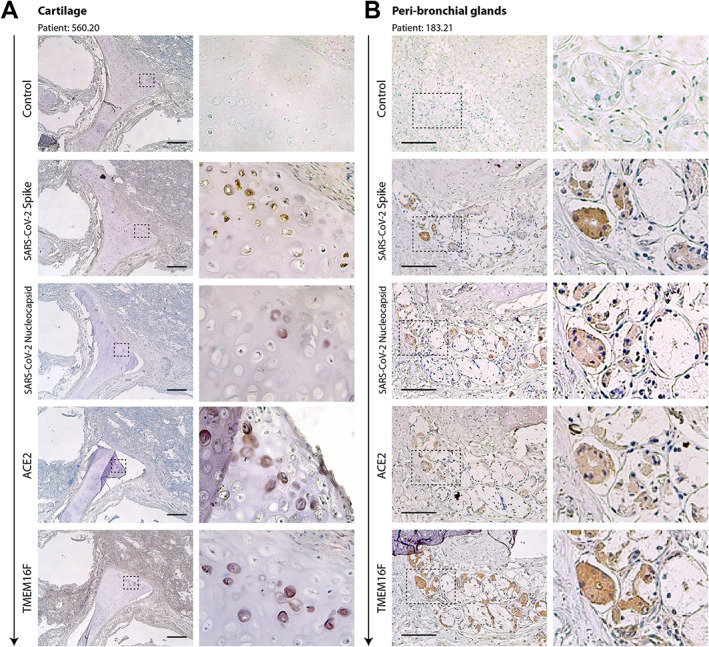
SARS-CoV-2 infection is clinically heterogeneous, ranging from asymptomatic to deadly. A few patients with COVID-19 appear to recover from acute viral infection but nevertheless progress in their disease and eventually die, despite persistent negativity at molecular tests for SARS-CoV-2 RNA. Here, we performed post-mortem analyses in 27 consecutive patients who had apparently recovered from COVID-19 but had progressively worsened in their clinical conditions despite repeated viral negativity in nasopharyngeal swabs or bronchioalveolar lavage for 11-300 consecutive days (average: 105.5 days). Three of these patients remained PCR-negative for over 9 months. Post-mortem analysis revealed evidence of diffuse or focal interstitial pneumonia in 23/27 (81%) patients, accompanied by extensive fibrotic substitution in 13 cases (47%). Despite apparent virological remission, lung pathology was similar to that observed in acute COVID-19 individuals, including micro- and macro-vascular thrombosis (67% of cases), vasculitis (24%), squamous metaplasia of the respiratory epithelium (30%), frequent cytological abnormalities and syncytia (67%), and the presence of dysmorphic features in the bronchial cartilage (44%). Consistent with molecular test negativity, SARS-CoV-2 antigens were not detected in the respiratory epithelium. In contrast, antibodies against both spike and nucleocapsid revealed the frequent (70%) infection of bronchial cartilage chondrocytes and para-bronchial gland epithelial cells. In a few patients (19%), we also detected positivity in vascular pericytes and endothelial cells. Quantitative RT-PCR amplification in tissue lysates confirmed the presence of viral RNA. Together, these findings indicate that SARS-CoV-2 infection can persist significantly longer than suggested by standard PCR-negative tests, with specific infection of specific cell types in the lung. Whether these persistently infected cells also play a pathogenic role in long COVID remains to be addressed. © 2023 The Authors. The Journal of Pathology published by John Wiley & Sons Ltd on behalf of The Pathological Society of Great Britain and Ireland.
Keywords: COVID-19; SARS-CoV-2; cartilage; nucleocapsid; parabronchial glands; post-mortem analysis; spike; syncytia.
© 2023 The Authors. The Journal of Pathology published by John Wiley & Sons Ltd on behalf of The Pathological Society of Great Britain and Ireland.
Figures
References
-
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID‐19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020; 323: 1239–1242. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
