

Is pain control for chronic neuropathic pain after inguinal hernia repair using endoscopic retroperitoneal neurectomy effective? A meta-analysis of 142 patients from 1995 to 2022
- PMID: 36652009
- PMCID: PMC9849289
- DOI: 10.1007/s00423-022-02748-6
Is pain control for chronic neuropathic pain after inguinal hernia repair using endoscopic retroperitoneal neurectomy effective? A meta-analysis of 142 patients from 1995 to 2022
Erratum in
-
Correction to: Langenbeck's Archives of Surgery Journal.Langenbecks Arch Surg. 2023 Feb 16;408(1):92. doi: 10.1007/s00423-023-02824-5. Langenbecks Arch Surg. 2023. PMID: 36792843 Free PMC article. No abstract available.
Abstract
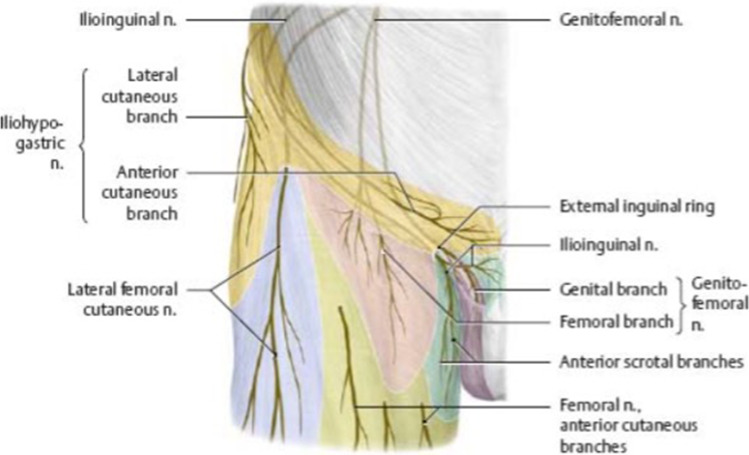
Purpose: Neuropathic pain is a complication after groin hernia surgery. Triple neurectomy of the iliohypogastric nerve, ilioinguinal nerve and genitofemoral nerve is an efficient treatment modality, with several surgical approaches. The minimally invasive endoscopic method to neurectomy was specifically investigated in this meta-analysis. Our aim is to determine the efficacy of this method in the treatment of chronic neuropathic pain posthernia repair surgery.
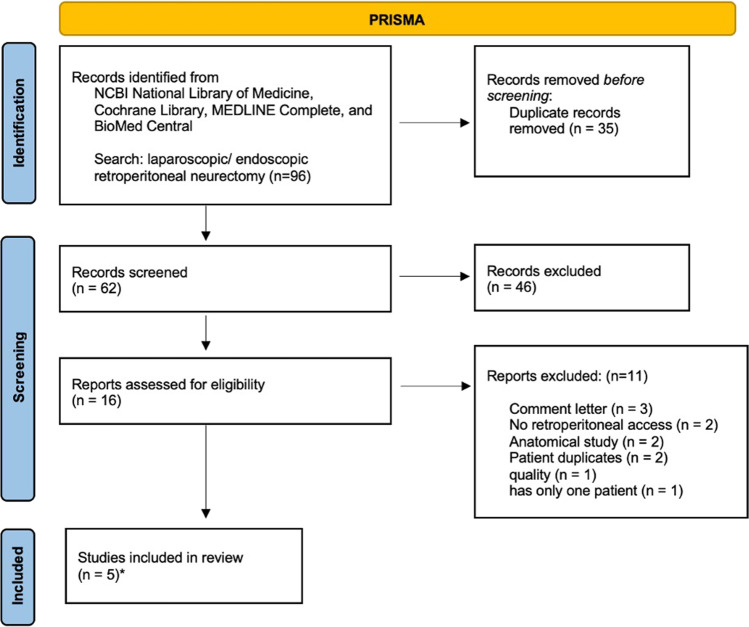
Methods: A systematic review was conducted using four databases to search for the keywords ("endoscopic retroperitoneal neurectomy" and "laparoscopic retroperitoneal neurectomy"). The NCBI National Library of Medicine, Cochrane Library, MEDLINE Complete and BioMed Central were last searched on 26 May 2022. Randomised control trials and retrospective or prospective papers involving endoscopic retroperitoneal neurectomy operations after inguinal hernia repair were included. All other surgeries, procedures and study designs were excluded. The internal quality of included studies was assessed using the Newcastle-Ottawa Scale. The percentage of patients who had reduction in pain ("positive treatment outcome") was used to assess the procedure's effectiveness in each analysis.
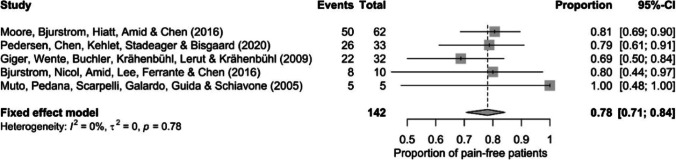
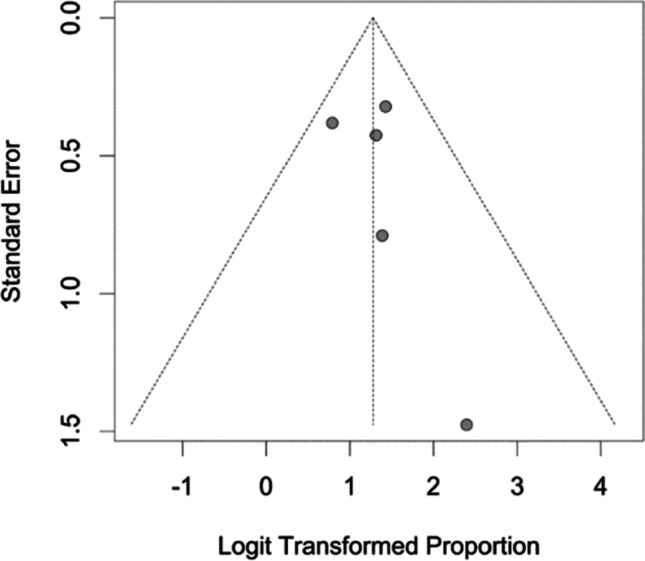
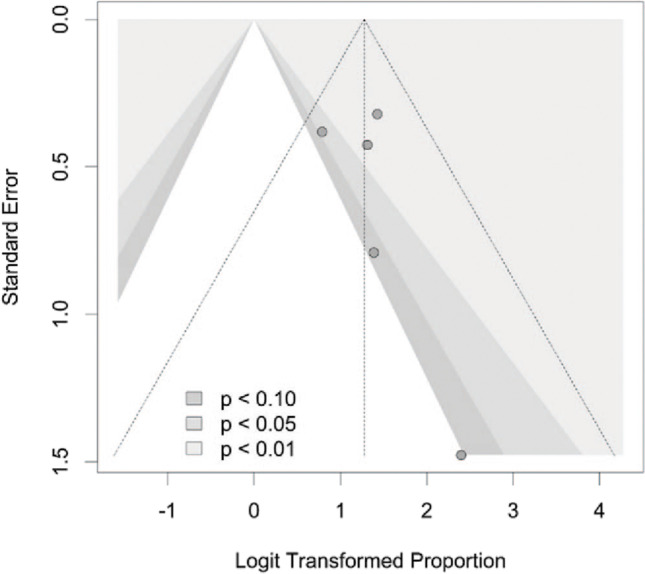
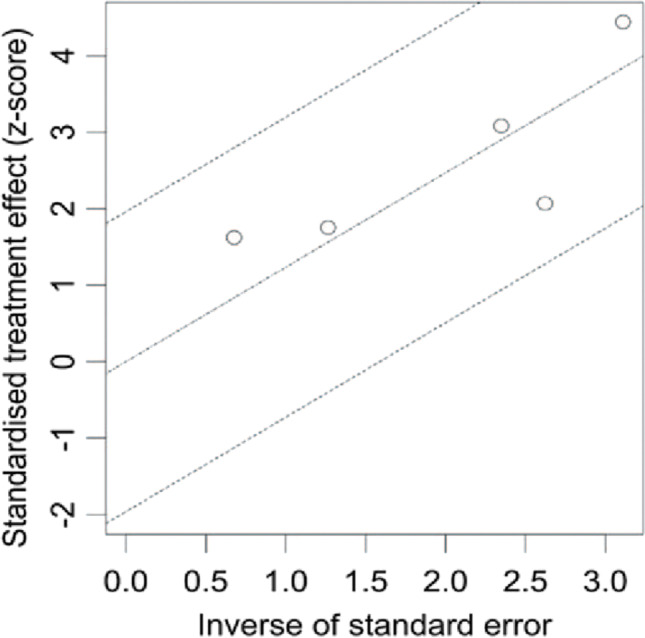
Results: Five comparable endoscopic retroperitoneal neurectomy studies with a total of 142 patients were analysed. Both the Wald test (Q (6) = 1.79, = .775) and the probability ratio test (Q (6) = 4.24, = .374) provide similar findings (0.000, 0.0% [0.0%; 78%]). The meta-analysis' key finding is that the intervention was up to 78% effective (95% confidence interval, 71%; 84%).
Conclusion: Endoscopic retroperitoneal neurectomy can be an effective treatment option for postoperative neuropathic pain relief following surgical hernia repair. Although there is limited reported experience with this technique, it may provide a clinical benefit to the patient. We recommend further prospective data and long-term follow-up studies be conducted to confirm and expand on these outcomes.
Keywords: Chronic neuropathic pain; Endoscopic approach; Hernia repair; Minimally invasive surgery; Retroperitoneal neurectomy.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Retroperitoneal Approach for Ilioinguinal, Iliohypogastric, and Genitofemoral Neurectomies in the Treatment of Refractory Groin Pain After Inguinal Hernia Repair.Ann Plast Surg. 2020 Apr;84(4):431-435. doi: 10.1097/SAP.0000000000002226. Ann Plast Surg. 2020. PMID: 32000253
-
Transabdominal laparoscopic retroperitoneal neurectomy for chronic pain after inguinal hernia repair and appendicectomy -a matched-pair study.BMC Surg. 2017 Jul 20;17(1):85. doi: 10.1186/s12893-017-0282-2. BMC Surg. 2017. PMID: 28728601 Free PMC article.
-
Impact of different neurectomy techniques on managing chronic pain after inguinal hernia repair: a meta-analysis and systematic review.Hernia. 2025 Aug 12;29(1):249. doi: 10.1007/s10029-025-03438-0. Hernia. 2025. PMID: 40794295 Free PMC article. Review.
-
Operative management of refractory neuropathic inguinodynia by a laparoscopic retroperitoneal approach.JAMA Surg. 2013 Oct;148(10):962-7. doi: 10.1001/jamasurg.2013.3189. JAMA Surg. 2013. PMID: 23903521
-
Nerve identification during open inguinal hernia repair: a systematic review and meta-analyses.Langenbecks Arch Surg. 2023 Oct 24;408(1):417. doi: 10.1007/s00423-023-03154-2. Langenbecks Arch Surg. 2023. PMID: 37874414 Free PMC article.
References
-
- Krähenbühl L, Striffeler H, Baer HU, Büchler MW. Retroperitoneal endoscopic neurectomy for nerve entrapment after hernia repair. Br J Surg. 1997;84:216–219. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
