

Effects of Mavacamten on Measures of Cardiopulmonary Exercise Testing Beyond Peak Oxygen Consumption: A Secondary Analysis of the EXPLORER-HCM Randomized Trial
- PMID: 36652223
- PMCID: PMC9857843
- DOI: 10.1001/jamacardio.2022.5099
Effects of Mavacamten on Measures of Cardiopulmonary Exercise Testing Beyond Peak Oxygen Consumption: A Secondary Analysis of the EXPLORER-HCM Randomized Trial
Abstract
Importance: Mavacamten, a cardiac myosin inhibitor, improved peak oxygen uptake (pVO2) in patients with symptomatic obstructive hypertrophic cardiomyopathy (HCM) in the EXPLORER-HCM study. However, the full extent of mavacamten's effects on exercise performance remains unclear.
Objective: To investigate the effect of mavacamten on exercise physiology using cardiopulmonary exercise testing (CPET).
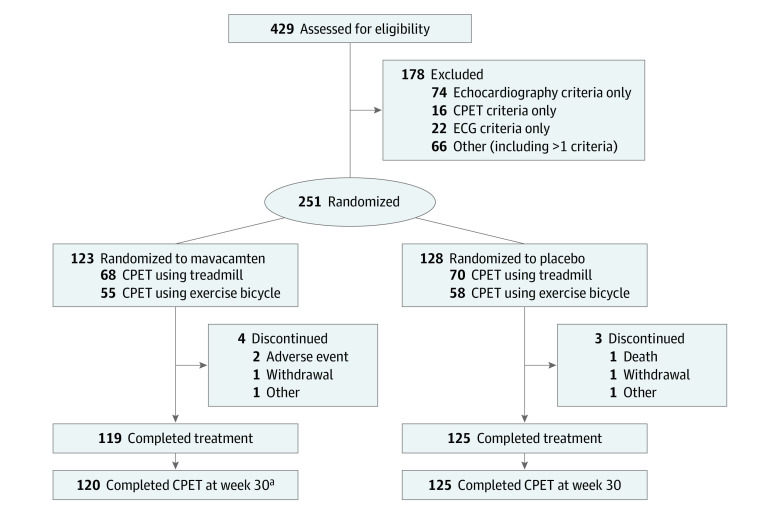
Design, setting, and participants: Exploratory analyses of the data from the EXPLORER-HCM study, a randomized, double-blind, placebo-controlled, phase 3 trial that was conducted in 68 cardiovascular centers in 13 countries. In total, 251 patients with symptomatic obstructive HCM were enrolled.
Interventions: Patients were randomly assigned in a 1:1 ratio to mavacamten or placebo.
Main outcomes and measures: The following prespecified exploratory cardiovascular and performance parameters were assessed with a standardized treadmill or bicycle ergometer test protocol at baseline and week 30: carbon dioxide output (VCO2), minute ventilation (VE), peak VE/VCO2 ratio, ventilatory efficiency (VE/VCO2 slope), peak respiratory exchange ratio (RER), peak circulatory power, ventilatory power, ventilatory threshold, peak metabolic equivalents (METs), peak exercise time, partial pressure of end-tidal carbon dioxide (PETCO2), and VO2/workload slope.
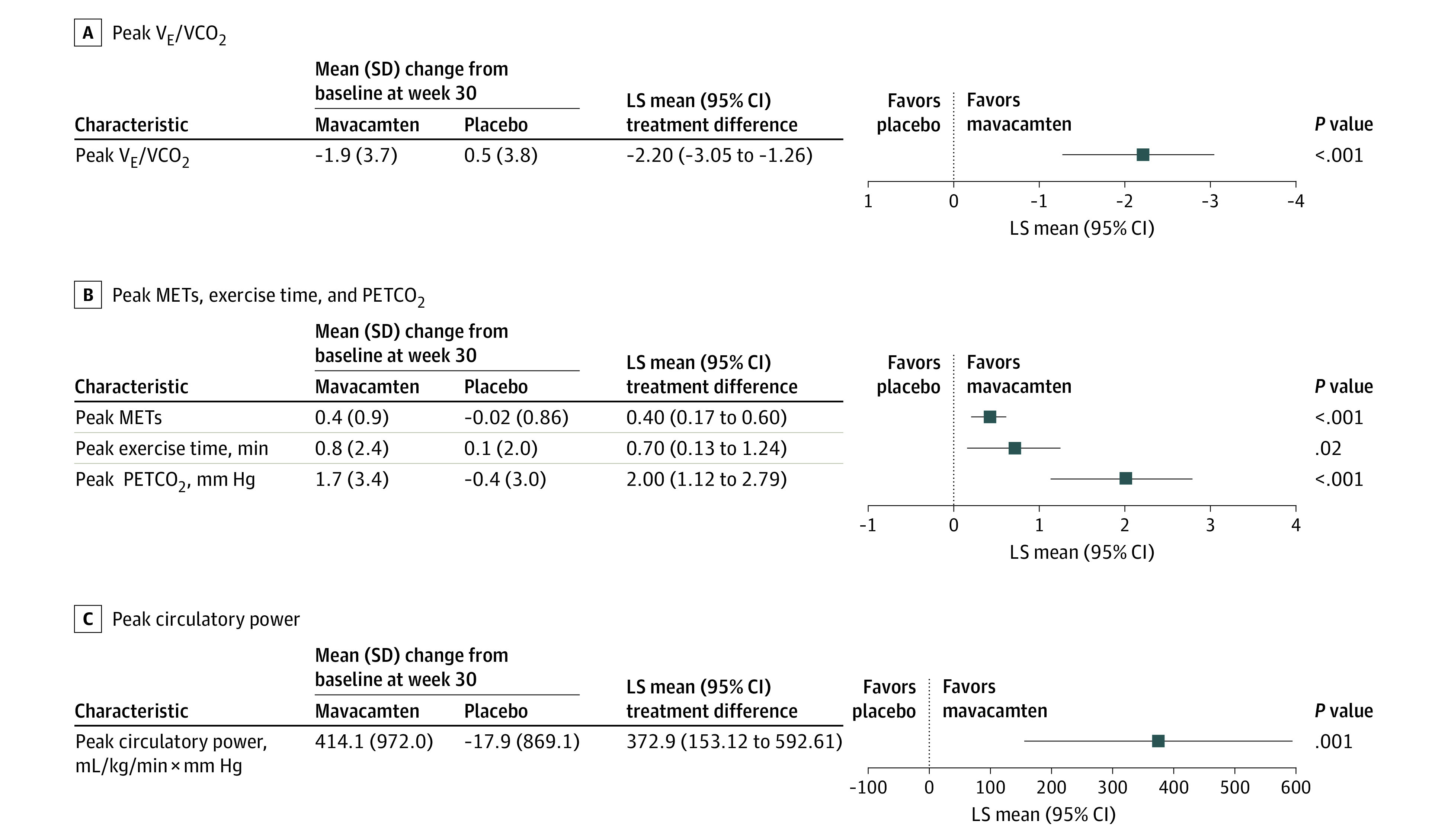
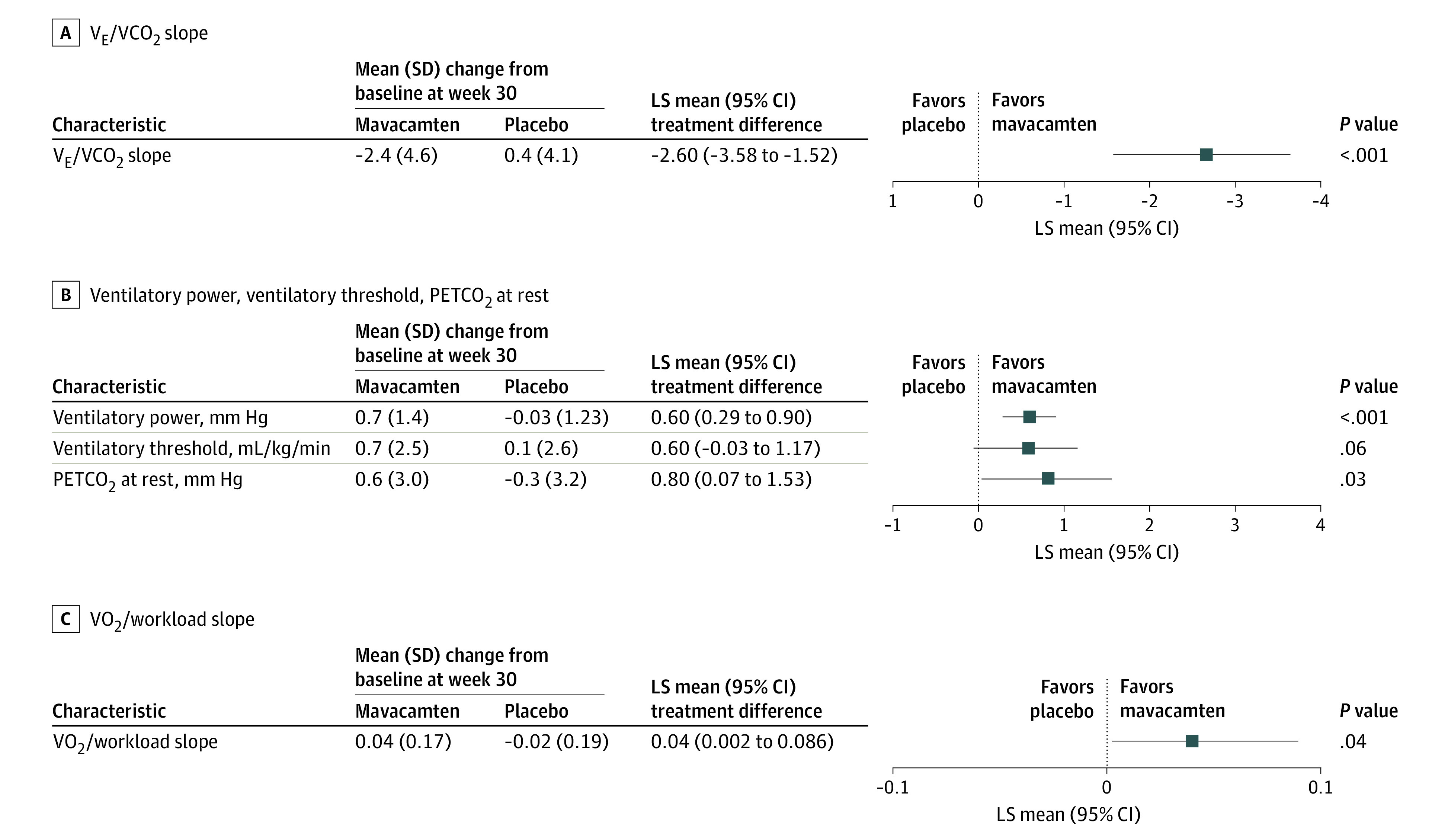
Results: Two hundred fifty-one patients were enrolled. The mean (SD) age was 58.5 (11.9) years and 59% of patients were male. There were significant improvements with mavacamten vs placebo in the following peak-exercise CPET parameters: peak VE/VCO2 ratio (least squares [LS] mean difference, -2.2; 95% CI, -3.05 to -1.26; P < .001), peak METs (LS mean difference, 0.4; 95% CI, 0.17-0.60; P < .001), peak circulatory power (LS mean difference, 372.9 mL/kg/min × mm Hg; 95% CI, 153.12-592.61; P = .001), and peak PETCO2 (LS mean difference, 2.0 mm Hg; 95% CI, 1.12-2.79; P < .001). Mavacamten also improved peak exercise time compared with placebo (LS mean difference, 0.7 minutes; 95% CI, 0.13-1.24; P = .02). There was a significant improvement in nonpeak-exercise CPET parameters, such as VE/VCO2 slope (LS mean difference, -2.6; 95% CI, -3.58 to -1.52; P < .001) and ventilatory power (LS mean difference, 0.6 mm Hg; 95% CI, 0.29-0.90; P < .001) favoring mavacamten vs placebo.
Conclusions and relevance: Mavacamten improved a range of CPET parameters beyond pVO2, indicating consistent and broad benefits on maximal exercise capacity. Although improvements in peak-exercise CPET parameters are clinically meaningful, the favorable effects of mavacamten on submaximal exertional tolerance provide further insights into the beneficial impact of mavacamten in patients with obstructive HCM.
Trial registration: ClinicalTrials.gov Identifier: NCT03470545.
Conflict of interest statement
Figures
Comment in
-
Assessment of Oxygen Pulse in Hypertrophic Cardiomyopathy-Reply.JAMA Cardiol. 2023 Aug 1;8(8):796-797. doi: 10.1001/jamacardio.2023.1889. JAMA Cardiol. 2023. PMID: 37405726 No abstract available.
-
Assessment of Oxygen Pulse in Hypertrophic Cardiomyopathy.JAMA Cardiol. 2023 Aug 1;8(8):795-796. doi: 10.1001/jamacardio.2023.1886. JAMA Cardiol. 2023. PMID: 37405753 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
