Rates of Follow-up Colonoscopy After a Positive Stool-Based Screening Test Result for Colorectal Cancer Among Health Care Organizations in the US, 2017-2020
- PMID: 36652246
- PMCID: PMC9856942
- DOI: 10.1001/jamanetworkopen.2022.51384
Rates of Follow-up Colonoscopy After a Positive Stool-Based Screening Test Result for Colorectal Cancer Among Health Care Organizations in the US, 2017-2020
Abstract
Importance: Noninvasive stool-based screening tests (SBTs) are effective alternatives to colonoscopy. However, a positive SBT result requires timely follow-up colonoscopy (FU-CY) to complete the colorectal cancer screening paradigm.
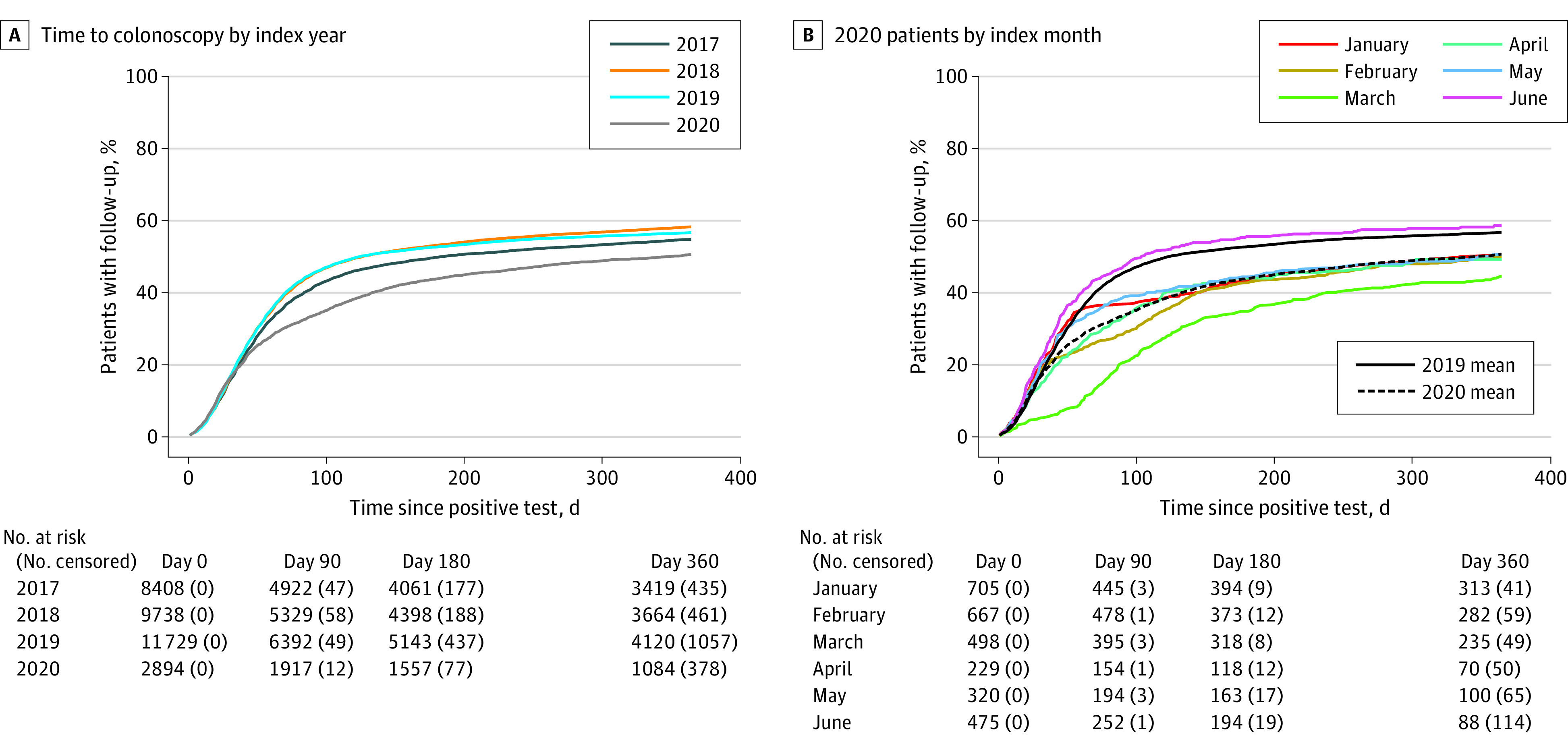
Objectives: To evaluate FU-CY rates after a positive SBT result and to assess the association of the early COVID-19 pandemic with FU-CY rates.
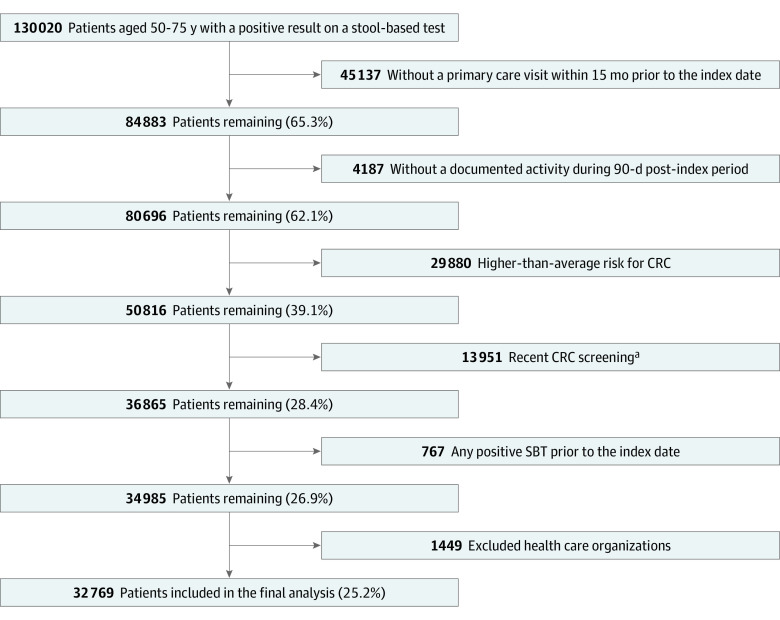
Design, setting, and participants: This mixed-methods cohort study included retrospective analysis of deidentified administrative claims and electronic health records data between June 1, 2015, and June 30, 2021, from the Optum Labs Data Warehouse and qualitative, semistructured interviews with clinicians from 5 health care organizations (HCOs). The study population included data from average-risk primary care patients aged 50 to 75 years with a positive SBT result between January 1, 2017, and June 30, 2020, at 39 HCOs.
Main outcomes and measures: The primary outcome was the FU-CY rate within 1 year of a positive SBT result according to patient age, sex, race, ethnicity, insurance type, Charlson Comorbidity Index (CCI), and prior SBT use.
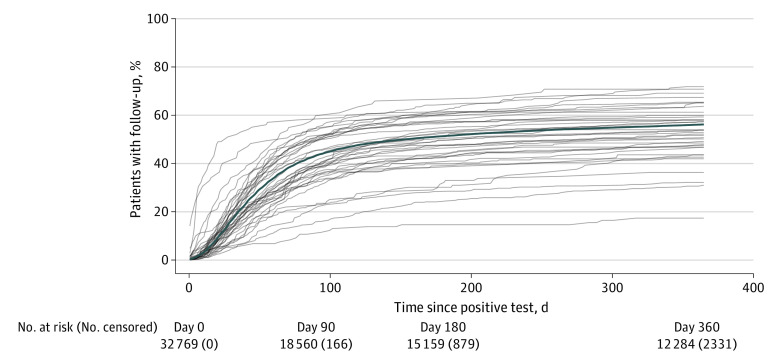
Results: This cohort study included 32 769 individuals (16 929 [51.7%] female; mean [SD] age, 63.1 [7.1] years; 2092 [6.4%] of Black and 28 832 [88.0%] of White race; and 825 [2.5%] of Hispanic ethnicity). The FU-CY rates were 43.3% within 90 days of the positive SBT result, 51.4% within 180 days, and 56.1% within 360 days (n = 32 769). In interviews, clinicians were uniformly surprised by the low FU-CY rates. Rates varied by race, ethnicity, insurance type, presence of comorbidities, and SBT used. In the Cox proportional hazards regression model, the strongest positive association was with multitarget stool DNA use (hazard ratio, 1.63 [95% CI, 1.57-1.68] relative to fecal immunochemical tests; P < .001), and the strongest negative association was with the presence of comorbidities (hazard ratio, 0.64 [95% CI, 0.59-0.71] for a CCI of >4 relative to 0; P < .001). The early COVID-19 pandemic was associated with lower FU-CY rates.
Conclusions and relevance: This study found that FU-CY rates after a positive SBT result for colorectal cancer screening were low among an average-risk population, with the median HCO achieving a 53.4% FU-CY rate within 1 year. Socioeconomic factors and the COVID-19 pandemic were associated with lower FU-CY rates, presenting opportunities for targeted intervention by clinicians and health care systems.
Conflict of interest statement
Figures