

Multicompartmental trauma alters bone marrow erythroblastic islands
- PMID: 36652391
- PMCID: PMC9877140
- DOI: 10.1097/TA.0000000000003821
Multicompartmental trauma alters bone marrow erythroblastic islands
Abstract
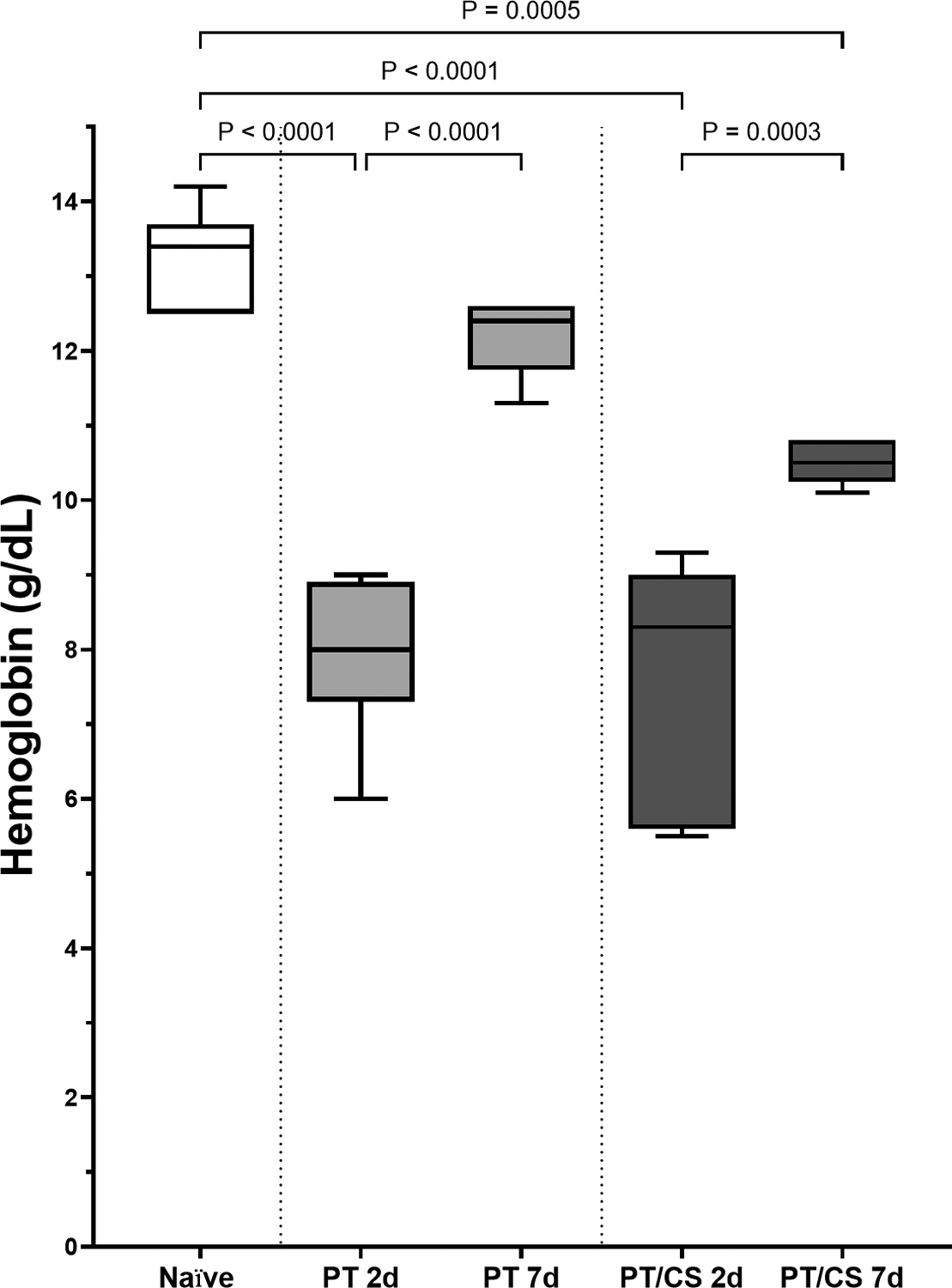
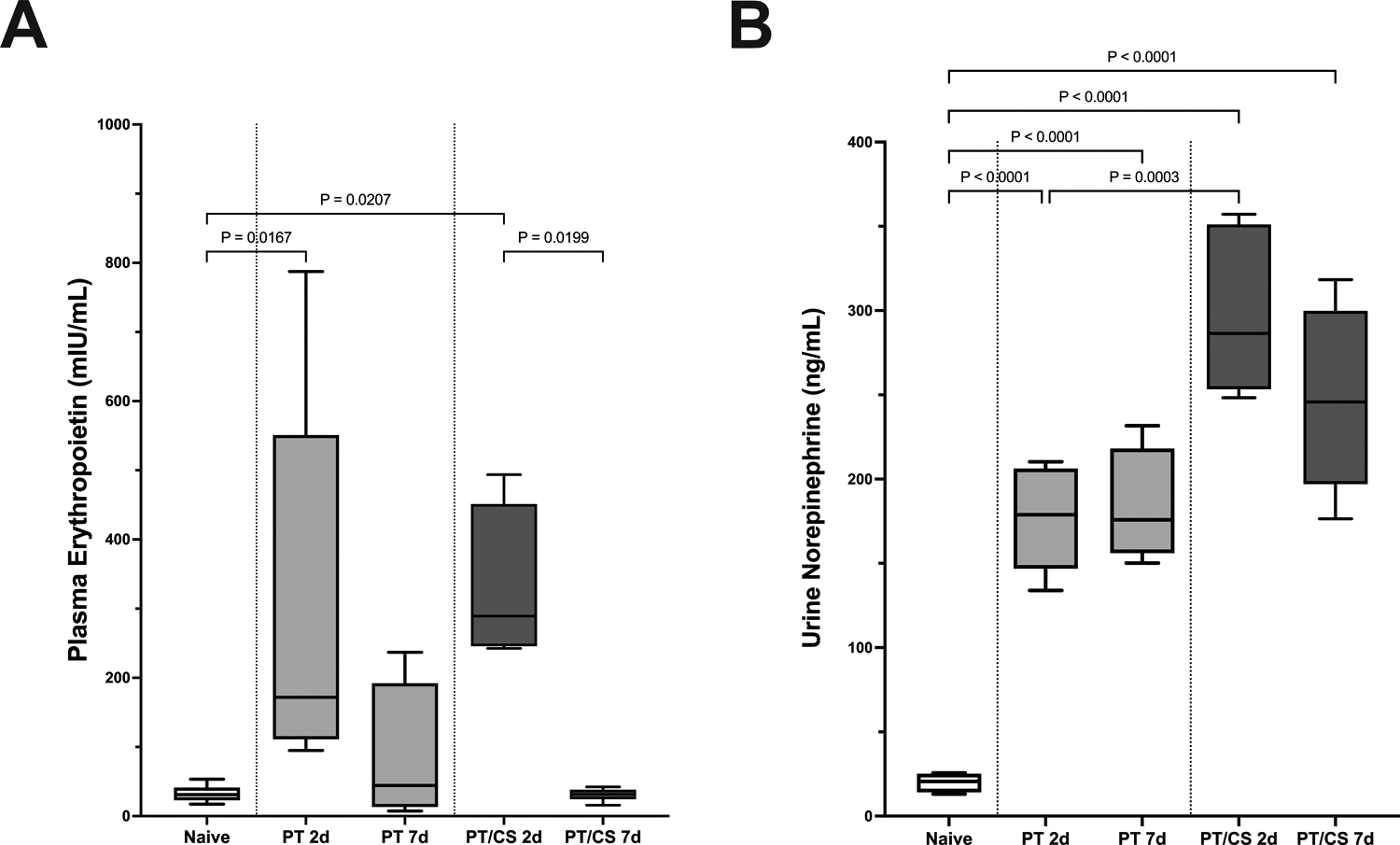
Background: Trauma is associated with widespread inflammation, neuroendocrine activation, and an inadequate bone marrow response to anemia. During late-stage erythropoiesis, erythroid progenitors/erythroblasts form clusters on the surface of specialized bone marrow macrophages where they are supported through terminal differentiation and enucleation. We hypothesized that these erythroblastic islands (EBIs) are adversely impacted by severe trauma.
Methods: Male Sprague-Dawley rats (n = 8/group) were subjected to either multiple injuries (PT) (lung contusion, hemorrhagic shock, cecectomy, and bifemoral pseudofractures), PT plus 2 hours of daily chronic restraint stress (PT/CS), or naive controls. Bone marrow was harvested on days 2 and 7. Nuclear-stained, enriched bone marrow EBIs were fixed and stained for CD71, VCAM-1, and CD163, and confocal images were obtained at 20 times magnification. Numbers of erythroid cells/EBI and ratio of reticulocytes/EBI were counted by a blinded observer. Differences were compared using analysis of variance, with significance defined as p < 0.05.
Results: PT and PT/CS had significantly reduced numbers of erythroid cells per EBI on day 2 when compared with naive (PT: 5.9 ± 1.0 cells [ p < 0.05], PT/CS: 6.8 ± 0.8 cells [ p < 0.05] vs. naive: 8.5 ± 0.8 cells). On day 7, the number of erythroid cells/EBI increased following PT (8.3 ± 0.4 cells) but remained reduced following PT/CS (5.9 ± 0.5 cells [ p < 0.05]). This correlated with an increased proportion of reticulocytes/EBI on day 7 following PT, which was not present following PT/CS (PT: 54% [ p < 0.05] vs. PT/CS: 28%).
Conclusion: Late-stage erythropoiesis was altered following multicompartmental PT early after injury, and these alterations persisted with the addition of daily chronic stress. Alterations in EBI structure and function after severe trauma and critical illness may serve as a promising new area of study to improve mechanistic understanding of persistent anemia after trauma.
Copyright © 2022 American Association for the Surgery of Trauma.
Conflict of interest statement
Disclosure Statement:
The authors report no proprietary, commercial or conflicts of interest in any product mentioned or concept discussed in this article.
Figures


References
-
- Corwin HL, Gettinger A, Pearl RG, Fink MP, Levy MM, Abraham E, et al. The CRIT Study: anemia and blood transfusion in the critically ill--current clinical practice in the United States. Crit Care Med. 2004;32(1):39–52. - PubMed
-
- Bateman AP, McArdle F, Walsh TS. Time course of anemia during six months follow up following intensive care discharge and factors associated with impaired recovery of erythropoiesis. Crit Care Med. 2009;37(6):1906–1912. - PubMed
-
- Walsh TS, Garrioch M, Maciver C, Lee RJ, MacKirdy F, McClelland DB, et al. Red cell requirements for intensive care units adhering to evidence-based transfusion guidelines. Transfusion. 2004; 44:1405–1411. - PubMed
-
- Charles A, Shaikh AA, Walters M, Huehl S, Pomerantz R. Blood transfusion is an independent predictor of mortality after blunt trauma. Am Surg. 2007;73(1):1–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
