

The impact of postoperative inclination of the joint line on clinical outcomes in total knee arthroplasty using a prosthesis with anatomical geometry
- PMID: 36653469
- PMCID: PMC9849260
- DOI: 10.1038/s41598-023-28182-2
The impact of postoperative inclination of the joint line on clinical outcomes in total knee arthroplasty using a prosthesis with anatomical geometry
Abstract
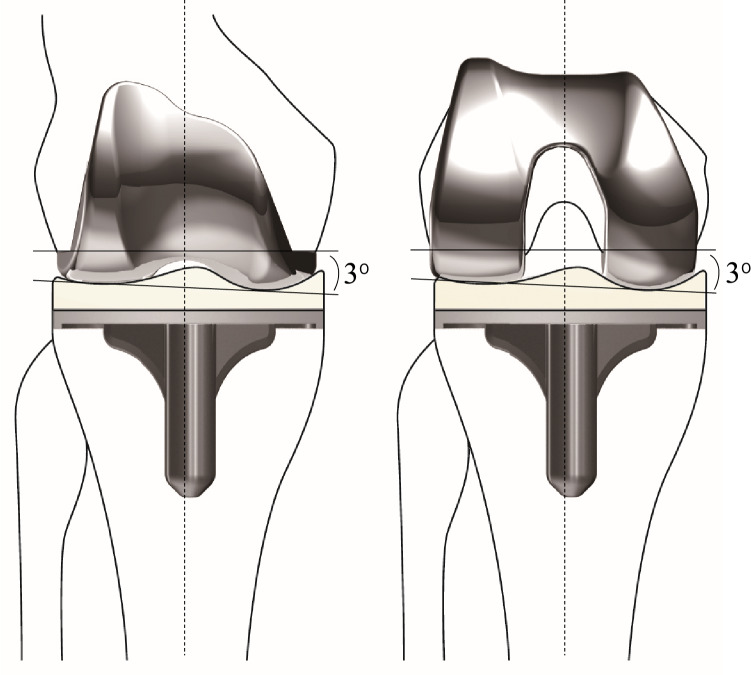
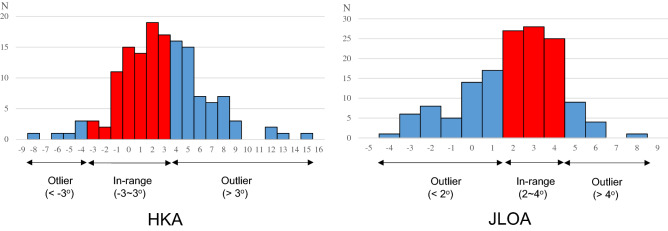
The goal of this study was to investigate the impact of postoperative inclination of the joint line on clinical results after total knee arthroplasty (TKA) using a prosthesis with anatomical geometry. This study included 145 primary cruciate-retaining type of knee prosthesis with anatomical geometry. Three years postoperatively, clinical outcomes including the patient-reported outcomes (PROs) were recorded. Limb alignment was evaluated by the hip-knee-ankle (HKA) axis and inclination of the joint line was assessed by the joint line orientation angle (JLOA). Knees were divided into two groups according to the HKA: in-range (- 3 to 3°) and outlier group (< - 3° or > 3°) or the JLOA: in-range (2-4°) and outlier group (< 2° or > 4°), and clinical outcomes were compared between the groups. Postoperative Knee Society Function Score (KS-FS) was significantly higher in the HKA in-range group than the outlier group (p = 0.01). The Knee Society Knee Score and all subscales of the Knee injury Osteoarthritis Outcome Score were comparable between the groups. A multivariate analysis revealed a significant association between age at operation and postoperative KS-FS > of 80 points. Neither HKA in-range nor JLOA in-range were associated with the higher knee function. In conclusion, TKA-postoperative inclination of the joint line was not relevant to the short-term PROs. Treatment strategies that attempt to make joint line inclination in order to improve postoperative PROs should be avoided, and alignment goals such as kinematic alignment should be considered carefully.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Baker PN, van der Meulen JH, Lewsey J, Gregg PJ. National Joint Registry for England and Wales. The role of pain and function in determining patient satisfaction after total knee replacement. Data from the National Joint Registry for England and Wales. J. Bone Jt. Surg. Br. 2007;89:893–900. doi: 10.1302/0301-620X.89B7.19091. - DOI - PubMed
-
- Howell SM, Kuznik K, Hull ML, Siston RA. Results of an initial experience with custom-fit positioning total knee arthroplasty in a series of 48 patients. Orthopedics. 2008;31(9):857–863. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
