

Acute phase characteristics and long-term complications of pulmonary embolism in COVID-19 compared to non-COVID-19 cohort: a large single-centre study
- PMID: 36653788
- PMCID: PMC9846660
- DOI: 10.1186/s12890-023-02323-9
Acute phase characteristics and long-term complications of pulmonary embolism in COVID-19 compared to non-COVID-19 cohort: a large single-centre study
Abstract
Background: To compare the severity of pulmonary embolism (PE) and the long-term complications between patients with and without COVID-19, and to investigate whether the tools for risk stratification of death are valid in this population.
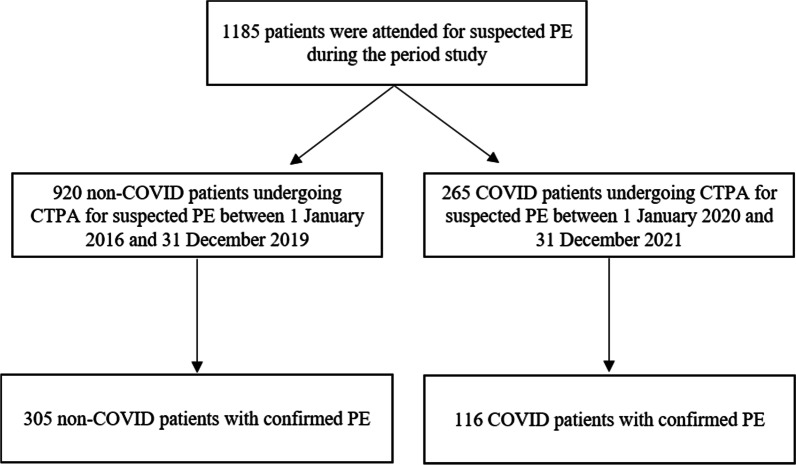
Methods: We retrospectively included hospitalized patients with PE from 1 January 2016 to 31 December 2022. Comparisons for acute episode characteristics, risk stratification of the PE, outcomes, and long-term complications were made between COVID and non-COVID patients.
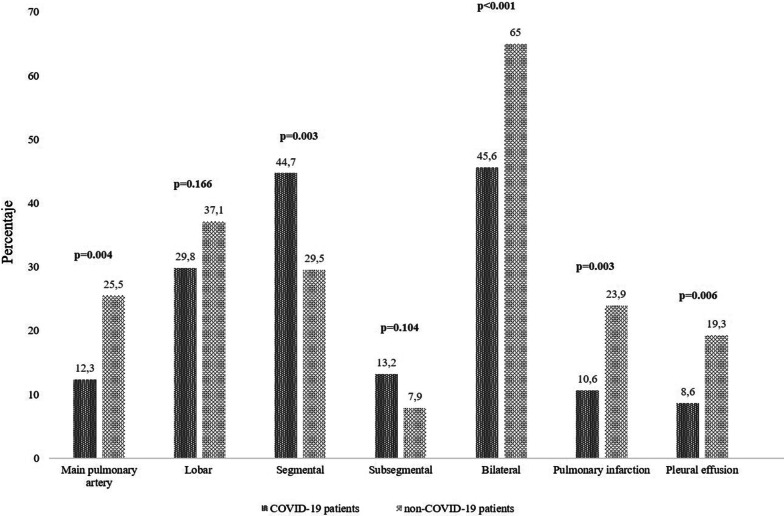
Results: We analyzed 116 (27.5%) COVID patients and 305 (72.4%) non-COVID patients. In patients with COVID-19, the traditional risk factors for PE were absent, and the incidence of deep vein thrombosis was lower. COVID patients showed significantly higher lymphocyte count, lactate dehydrogenase, lactic acid, and D-dimer levels. COVID patients had PE of smaller size (12.3% vs. 25.5% main pulmonary artery, 29.8% vs. 37.1% lobar, 44.7% vs. 29.5% segmental and 13.2% vs. 7.9% subsegmental, respectively; p < 0.001), less right ventricular dysfunction (7.7% vs. 17.7%; p = 0.007) and higher sPESI score (1.66 vs. 1.11; p < 0.001). The need for mechanical ventilation was significantly higher in COVID patients (8.6% vs. 1.3%; p < 0.001); However, the in-hospital death was less (5.2% vs. 10.8%; p = 0.074). The incidence of long-term complications was lower in COVID cohort (p < 0.001). PE severity assessed by high sPESI and intermediate and high-risk categories were independently associated with in-hospital mortality in COVID patients.
Conclusion: The risk of in-hospital mortality and the incidence of long-term complications were lower in COVID-19. The usual tools for risk stratification of PE are valid in COVID patients.
Keywords: COVID-19; Case-control study; Long-term complications; Pulmonary embolism; Risk stratification; Severity.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Klok FA, Kruip MJHA, van der Meer NJM, Arbous MS, Gommers D, Kant KM, et al. Confirmation of the high cumulative incidence of thrombotic complications in critically ill ICU patients with COVID-19: an updated analysis. Thromb Res. 2020;191:148–50. doi: 10.1016/j.thromres.2020.04.041. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
