

The prediction of in-hospital mortality in chronic kidney disease patients with coronary artery disease using machine learning models
- PMID: 36653875
- PMCID: PMC9847092
- DOI: 10.1186/s40001-023-00995-x
The prediction of in-hospital mortality in chronic kidney disease patients with coronary artery disease using machine learning models
Abstract
Objective: Chronic kidney disease (CKD) patients with coronary artery disease (CAD) in the intensive care unit (ICU) have higher in-hospital mortality and poorer prognosis than patients with either single condition. The objective of this study is to develop a novel model that can predict the in-hospital mortality of that kind of patient in the ICU using machine learning methods.
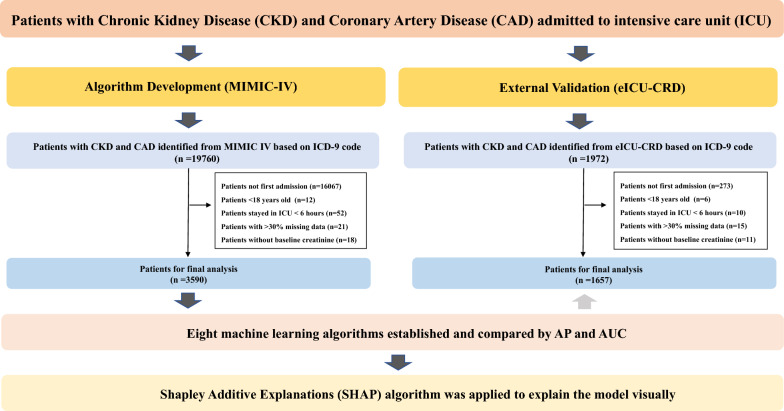
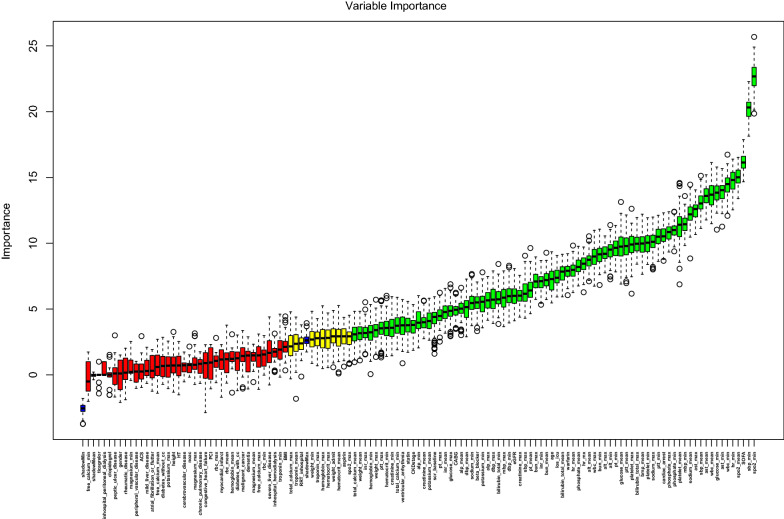
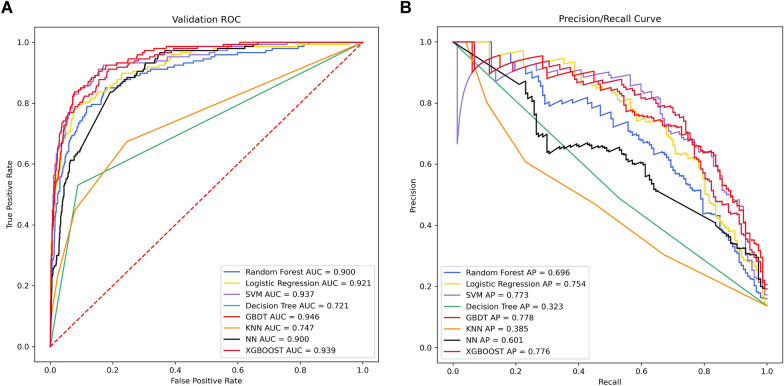
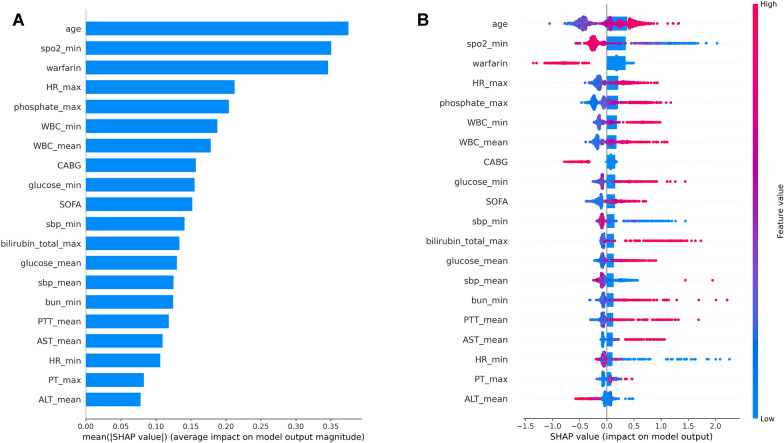
Methods: Data of CKD patients with CAD were extracted from the Medical Information Mart for Intensive Care IV (MIMIC-IV) database. Boruta algorithm was conducted for the feature selection process. Eight machine learning algorithms, such as logistic regression (LR), random forest (RF), Decision Tree, K-nearest neighbors (KNN), Gradient Boosting Decision Tree Machine (GBDT), Support Vector Machine (SVM), Neural Network (NN), and Extreme Gradient Boosting (XGBoost), were conducted to construct the predictive model for in-hospital mortality and performance was evaluated by average precision (AP) and area under the receiver operating characteristic curve (AUC). Shapley Additive Explanations (SHAP) algorithm was applied to explain the model visually. Moreover, data from the Telehealth Intensive Care Unit Collaborative Research Database (eICU-CRD) were acquired as an external validation set.
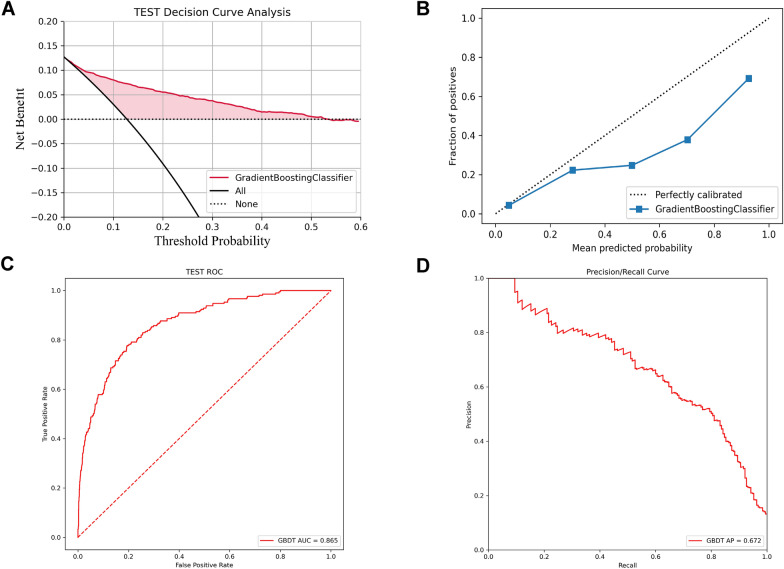
Results: 3590 and 1657 CKD patients with CAD were acquired from MIMIC-IV and eICU-CRD databases, respectively. A total of 78 variables were selected for the machine learning model development process. Comparatively, GBDT had the highest predictive performance according to the results of AUC (0.946) and AP (0.778). The SHAP method reveals the top 20 factors based on the importance ranking. In addition, GBDT had good predictive value and a certain degree of clinical value in the external validation according to the AUC (0.865), AP (0.672), decision curve analysis, and calibration curve.
Conclusion: Machine learning algorithms, especially GBDT, can be reliable tools for accurately predicting the in-hospital mortality risk for CKD patients with CAD in the ICU. This contributed to providing optimal resource allocation and reducing in-hospital mortality by tailoring precise management and implementation of early interventions.
Keywords: Chronic kidney disease; Coronary artery disease; In-hospital mortality; MIMIC-IV database; Machine learning.
© 2023. The Author(s).
Conflict of interest statement
Not applicable.
Figures
Similar articles
-
Interpretable machine learning model for early prediction of 28-day mortality in ICU patients with sepsis-induced coagulopathy: development and validation.Eur J Med Res. 2024 Jan 3;29(1):14. doi: 10.1186/s40001-023-01593-7. Eur J Med Res. 2024. PMID: 38172962 Free PMC article.
-
Interpretable machine learning for 28-day all-cause in-hospital mortality prediction in critically ill patients with heart failure combined with hypertension: A retrospective cohort study based on medical information mart for intensive care database-IV and eICU databases.Front Cardiovasc Med. 2022 Oct 12;9:994359. doi: 10.3389/fcvm.2022.994359. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36312291 Free PMC article.
-
[Constructing a predictive model for the death risk of patients with septic shock based on supervised machine learning algorithms].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024 Apr;36(4):345-352. doi: 10.3760/cma.j.cn121430-20230930-00832. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024. PMID: 38813626 Chinese.
-
The CMLA score: A novel tool for early prediction of renal replacement therapy in patients with cardiogenic shock.Curr Probl Cardiol. 2024 Dec;49(12):102870. doi: 10.1016/j.cpcardiol.2024.102870. Epub 2024 Sep 27. Curr Probl Cardiol. 2024. PMID: 39343053 Review.
-
Machine learning algorithms' accuracy in predicting kidney disease progression: a systematic review and meta-analysis.BMC Med Inform Decis Mak. 2022 Aug 1;22(1):205. doi: 10.1186/s12911-022-01951-1. BMC Med Inform Decis Mak. 2022. PMID: 35915457 Free PMC article.
Cited by
-
RNA‑seq analysis of predictive markers associated with glutamine metabolism in thyroid cancer.Mol Med Rep. 2025 Jun;31(6):145. doi: 10.3892/mmr.2025.13510. Epub 2025 Apr 4. Mol Med Rep. 2025. PMID: 40183409 Free PMC article.
-
Association of Liver Fibrosis Markers with Mortality Outcomes in Patients with Chronic Kidney Disease and Coronary Artery Disease: Insights from the NHANES 1999-2018 Data.Cardiorenal Med. 2025;15(1):153-163. doi: 10.1159/000543500. Epub 2025 Jan 21. Cardiorenal Med. 2025. PMID: 39837280 Free PMC article.
-
Development and Validation of Machine Learning Models for Predicting 7-Day Mortality in Critically Ill Patients with Traumatic Spinal Cord Injury: A Multicenter Retrospective Study.Neurocrit Care. 2025 Jun 25. doi: 10.1007/s12028-025-02308-y. Online ahead of print. Neurocrit Care. 2025. PMID: 40563047
-
A deep learning model for clinical outcome prediction using longitudinal inpatient electronic health records.JAMIA Open. 2025 Apr 10;8(2):ooaf026. doi: 10.1093/jamiaopen/ooaf026. eCollection 2025 Apr. JAMIA Open. 2025. PMID: 40213364 Free PMC article.
-
Comprehensive Analysis Based on Genes Associated With Cuproptosis, Ferroptosis, and Pyroptosis for the Prediction of Diagnosis and Therapies in Coronary Artery Disease.Cardiovasc Ther. 2025 Mar 15;2025:9106621. doi: 10.1155/cdr/9106621. eCollection 2025. Cardiovasc Ther. 2025. PMID: 40124544 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
