

Spiliotis-Farfarelos Maneuver for the Management of Small Bowel Obstruction and Frozen Pelvis in Patients With Peritoneal Metastasis
- PMID: 36654562
- PMCID: PMC9838686
- DOI: 10.7759/cureus.32518
Spiliotis-Farfarelos Maneuver for the Management of Small Bowel Obstruction and Frozen Pelvis in Patients With Peritoneal Metastasis
Abstract
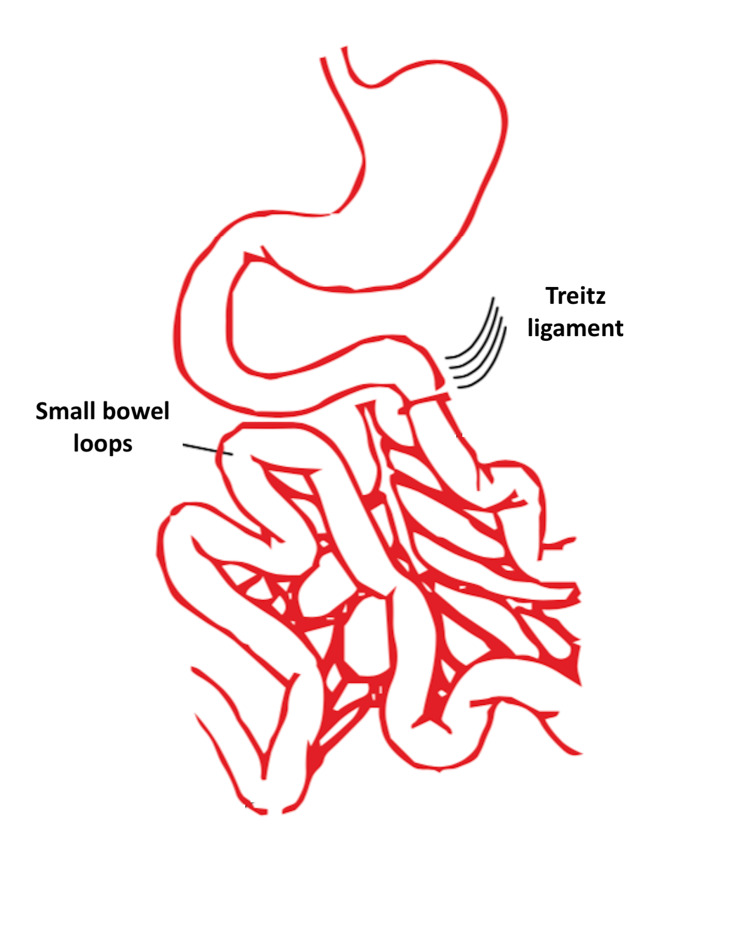
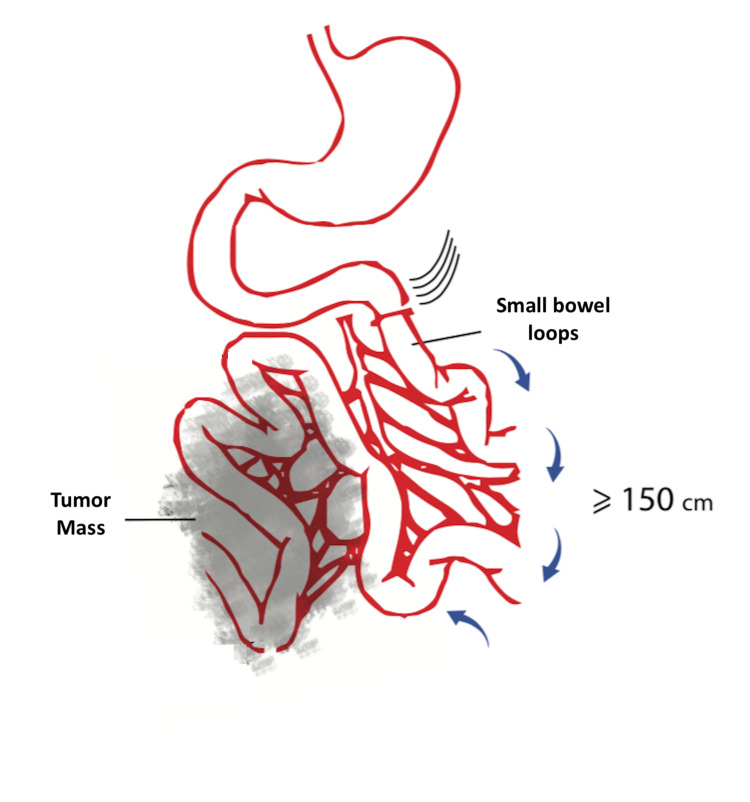
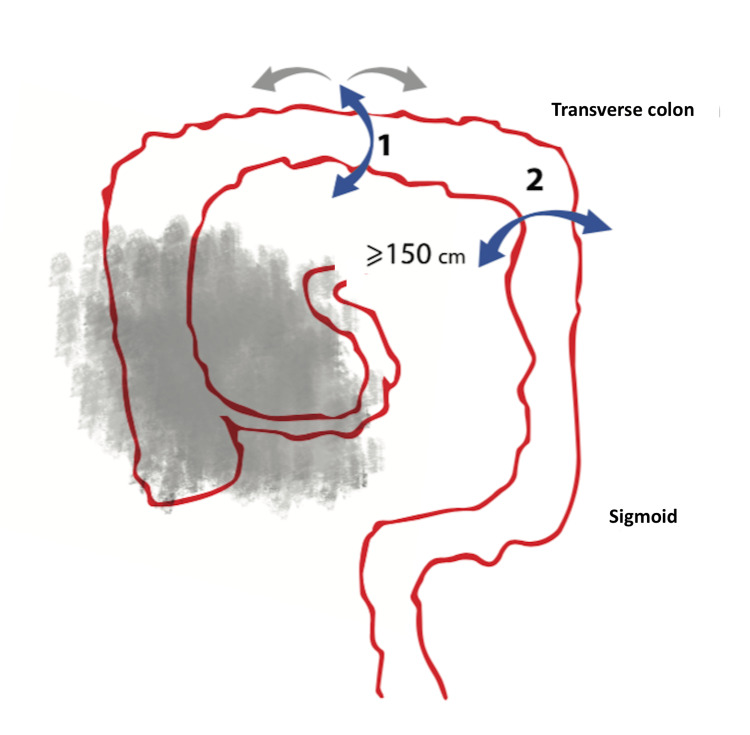
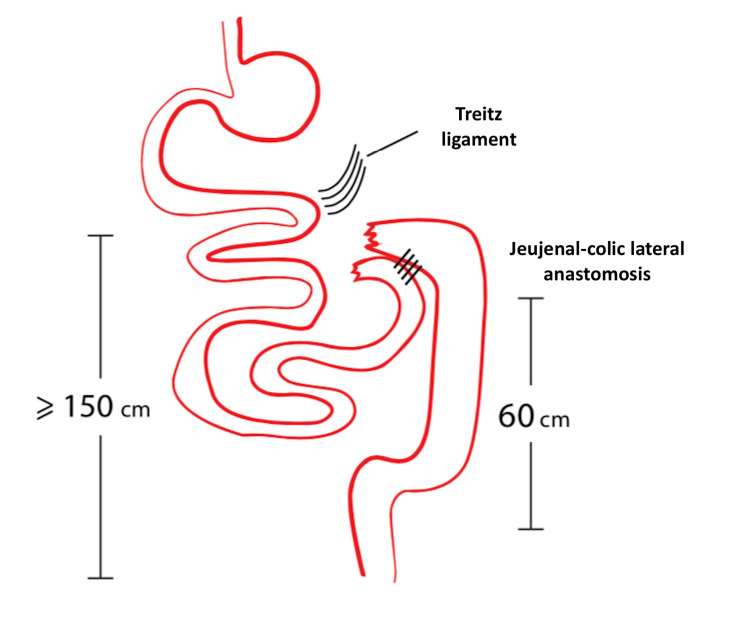
The management of the advanced peritoneal disease is demanding especially in cases of extensive bowel infiltration and the obstruction of the gastrointestinal tract in different sites. Patients with bowel obstruction due to peritoneal carcinomatosis have an overall survival that ranges from three to eight months to four to five weeks based on the operability or not of the disease, respectively. The decision to operate should carefully consider the balance between the probability of symptomatic relief and the risk of severe perioperative complications and survival after surgery. The extent of the disease and postoperative malnutrition could further complicate patients' postoperative course. We aim to present an operative maneuver of bowel preparation and fixation in cases of extensive infiltration of the small bowel by peritoneal carcinomatosis (PC) in order to eliminate the risk of postoperative fistula formation or anastomotic leakage.
Keywords: advanced gynecological cancer; cytoreduction; gastrointestinal cancer; peritoneal carcinomatosis; surgical maneuver.
Copyright © 2022, Spiliotis et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Palliative surgery as a bridge to systemic treatment for malignant bowel obstruction due to peritoneal metastases: a retrospective, case-control study [IN PRESS] Razak OA, Yang SY, Cho MS, Min BS, Han YD. Asian J Surg. 2022 - PubMed
LinkOut - more resources
Full Text Sources