

Knowledge, attitudes, and practices towards HPV vaccination among reproductive age women in a HIV hotspot in the US
- PMID: 36656804
- PMCID: PMC9851547
- DOI: 10.1371/journal.pone.0275141
Knowledge, attitudes, and practices towards HPV vaccination among reproductive age women in a HIV hotspot in the US
Abstract
Background: Human papillomavirus (HPV) is the most common sexually transmitted infection (STI) in the US, responsible for cervical cancer and increased risk of Human Immunodeficiency Virus (HIV) acquisition. Despite an effective HPV vaccine, women's HPV vaccination coverage and rates remain far below desired levels. This study aimed to evaluate HPV knowledge, attitudes, and vaccination practices as well as factors associated with HPV vaccination among women of reproductive age living in Miami, Florida, a Southern US city with a high incidence of STIs and low HPV vaccination coverage.
Methods: From April to June 2022, 100 HIV-negative, cisgender, sexually active women aged 18-45 years were recruited from the Miami community. Participants completed validated questionnaires using REDCap© electronic surveys, assessing socio-demographics and sexual behaviors; HPV knowledge, screening, vaccination practices; barriers and motivators to HPV vaccination. A cumulative HPV knowledge score (HPV score) was generated. Factors associated with HPV vaccination were analyzed by Chi-square, Fisher's exact test, studentized t-test, and multivariate logistic regression (MLR).
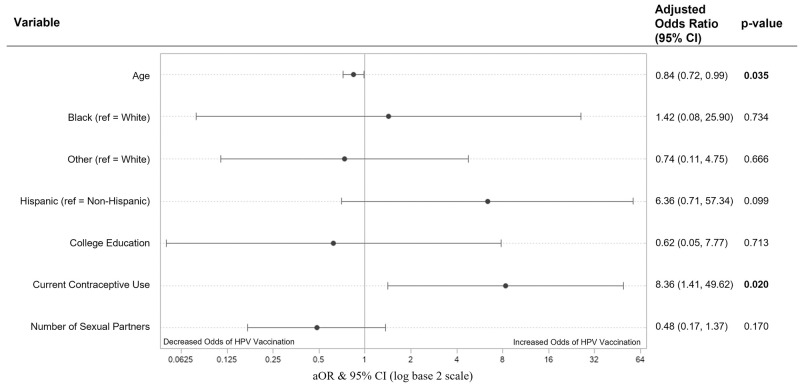
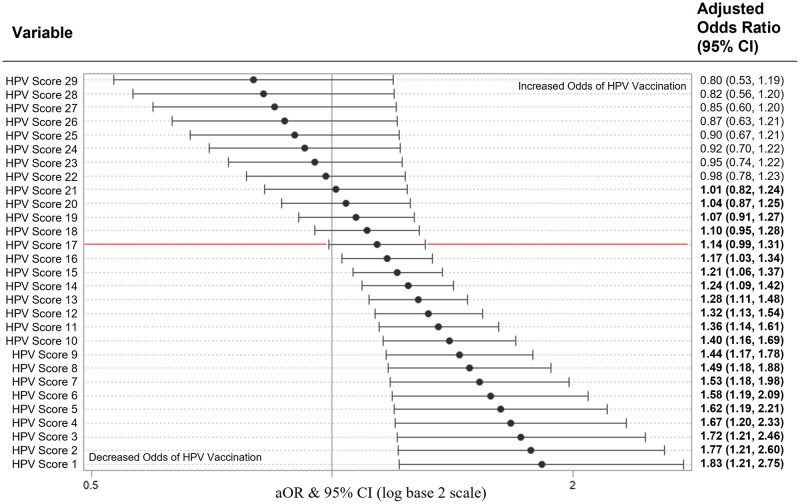
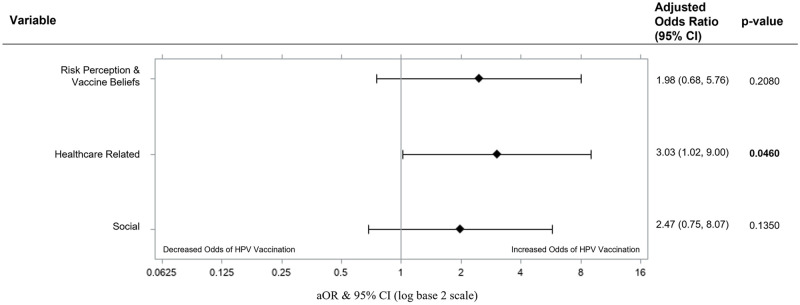
Results: A total of 100 participants were enrolled, and 84 who knew their vaccination status were included in the analysis. Of these, 43 reported receiving at least 1 HPV vaccine dose (vaccinated group) and 41 reported never being vaccinated (unvaccinated group). Mean age was 24.7 (SD 4.03) years for the vaccinated group and 31.4 (SD 8.33) for the unvaccinated group. Mean HPV score was 18.9/29 (SD 6.05) for the vaccinated group and 9.1/29 (SD 8.82) for the unvaccinated group. Amongst vaccinated participants, 76.74% reported a history of HPV/Pap smear screening vs 87.80% in the unvaccinated group. Barriers to HPV vaccination included: 14.6% low-risk perception, 29.3% healthcare barriers, and 46.3% vaccine hesitancy and personal beliefs. Motivators t HPV vaccination included: risk perception and vaccine beliefs (71.42%), healthcare-related (60.71%) and social motivators (55.95%). In the first MLR, one-point increases in HPV score were significantly associated with higher odds of HPV vaccination until an HPV score of 16, and a one-year increase in age was associated with a 16% lower odds of HPV vaccination (aOR = 0.84, 95% CI [0.72, 0.99]; p = 0.035). Contraception use was also associated with HPV vaccination (aOR 8.36 (95% CI [1.41, 49.62]; p = 0.020). Race, ethnicity, college education status, and number of sexual partners were not significant predictors of HPV vaccination. In the second MLR evaluating vaccination motivators as predictors of HPV vaccination, we found that individuals who were motivated by healthcare had 3.03 (95% CI [1.02, 9.00]; p = 0.046) times the odds of HPV vaccination compared to individuals without healthcare-related motivators.
Conclusion: Findings suggest suboptimal HPV knowledge and low vaccination rates among women of reproductive age. Public health efforts should focus on increasing basic HPV knowledge among women with little-to-no HPV knowledge to increase vaccine uptake.
Copyright: © 2023 Villavicencio et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Centers for Disease Control and Prevention (CDC). QuickStats: Percentage of Adults Aged 18–26 Years Who Ever Received a Human Papillomavirus Vaccine, by Race and Hispanic Origin and Sex—National Health Interview Survey, United States, 2019. MMWR and Morbidity and Mortality Weekly Report, 2021. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
