

Using patient-derived organoids to predict locally advanced or metastatic lung cancer tumor response: A real-world study
- PMID: 36657446
- PMCID: PMC9975107
- DOI: 10.1016/j.xcrm.2022.100911
Using patient-derived organoids to predict locally advanced or metastatic lung cancer tumor response: A real-world study
Abstract
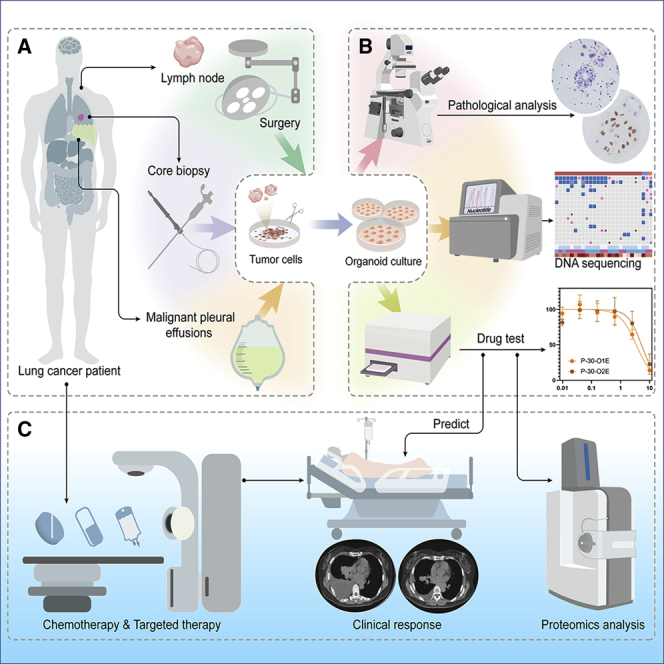
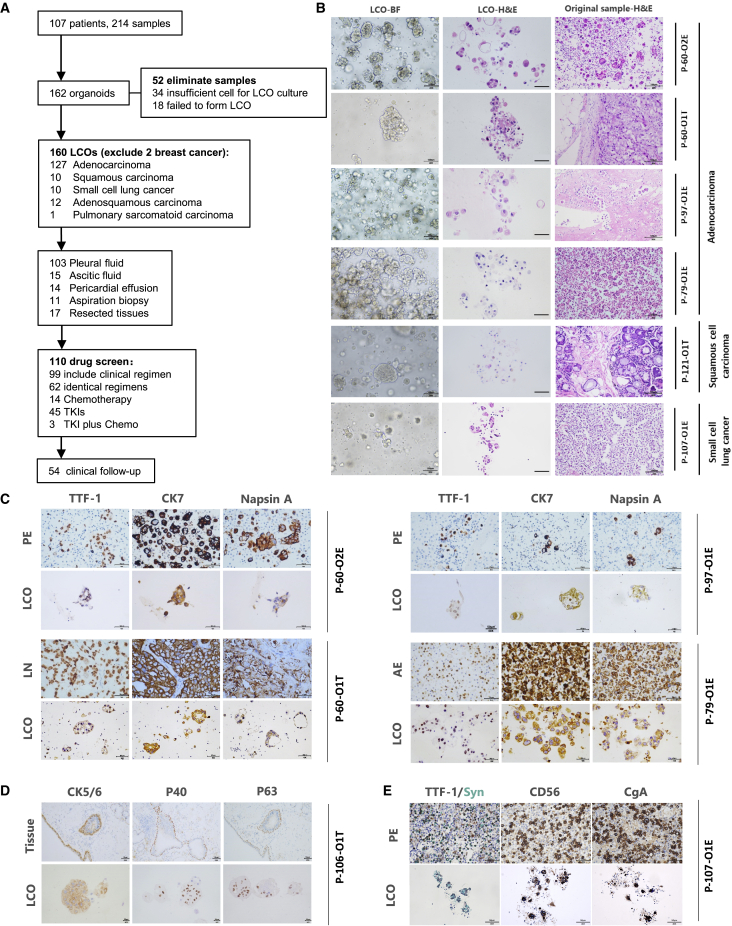
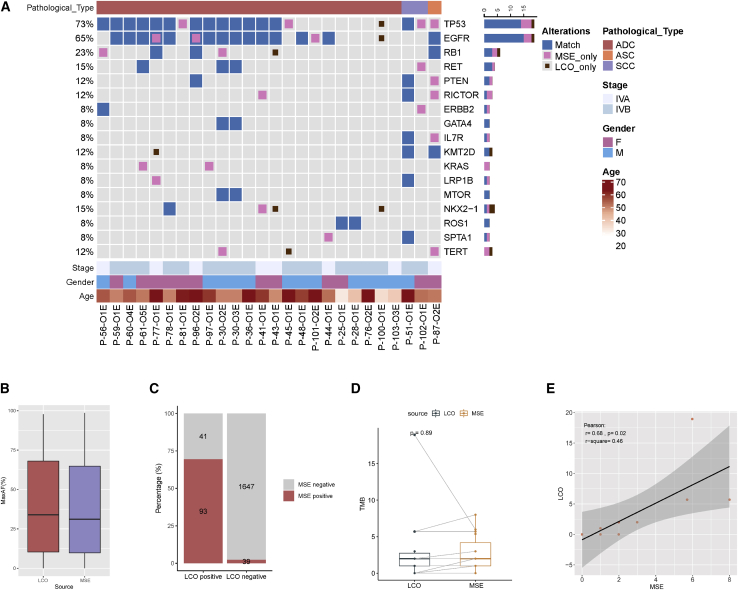
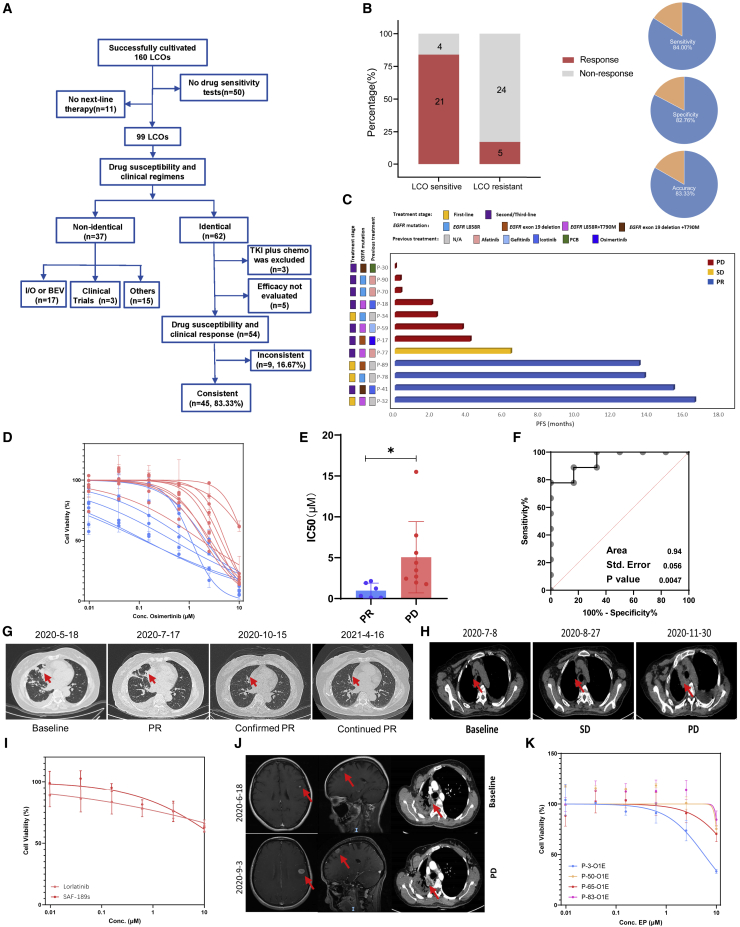
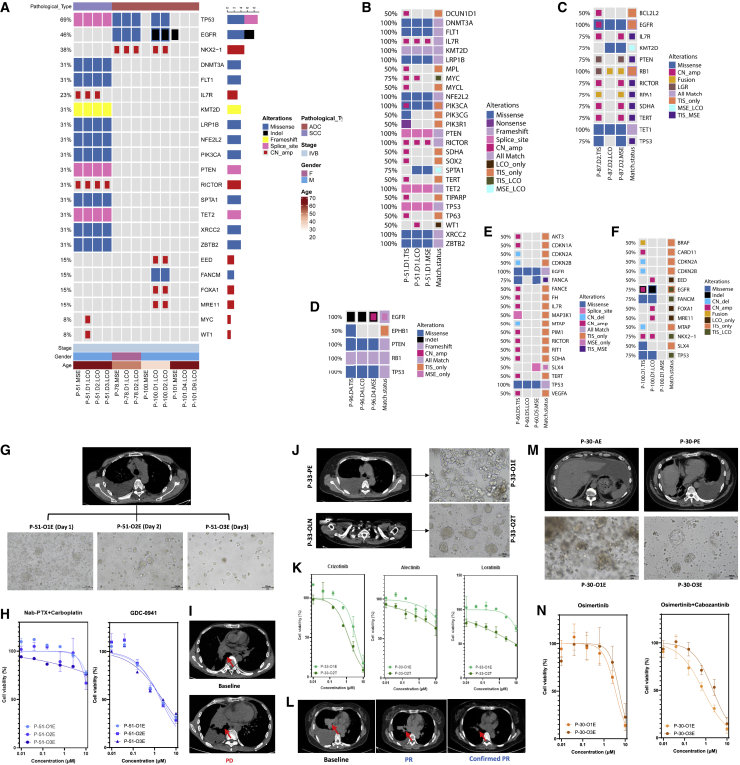
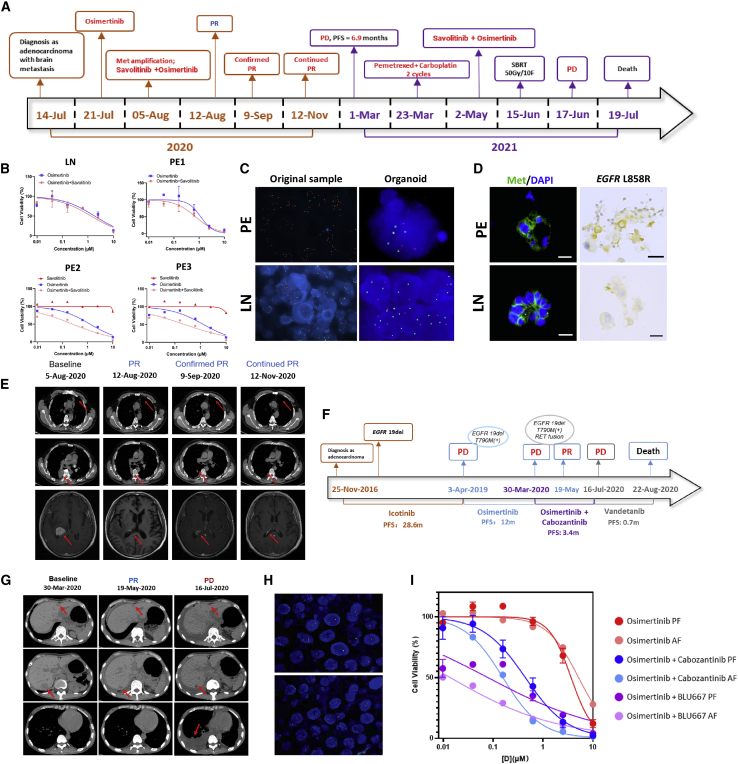
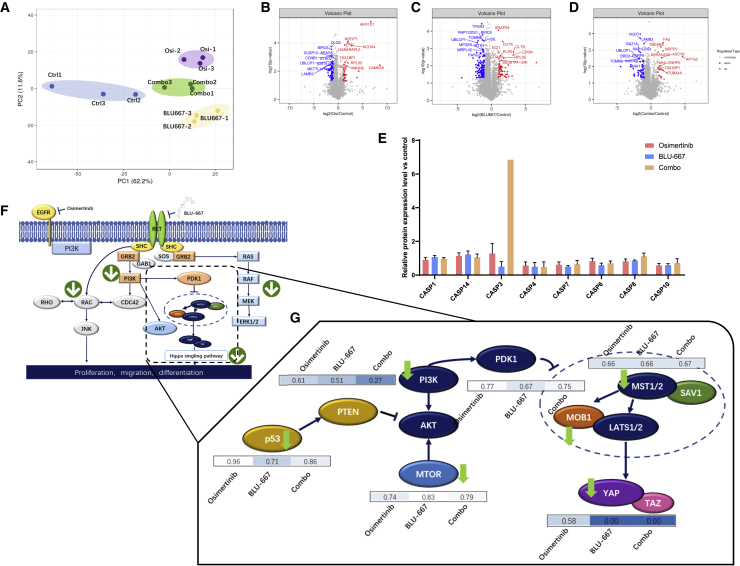
Predicting the clinical response to chemotherapeutic or targeted treatment in patients with locally advanced or metastatic lung cancer requires an accurate and affordable tool. Tumor organoids are a potential approach in precision medicine for predicting the clinical response to treatment. However, their clinical application in lung cancer has rarely been reported because of the difficulty in generating pure tumor organoids. In this study, we have generated 214 cancer organoids from 107 patients, of which 212 are lung cancer organoids (LCOs), primarily derived from malignant serous effusions. LCO-based drug sensitivity tests (LCO-DSTs) for chemotherapy and targeted therapy have been performed in a real-world study to predict the clinical response to the respective treatment. LCO-DSTs accurately predict the clinical response to treatment in this cohort of patients with advanced lung cancer. In conclusion, LCO-DST is a promising precision medicine tool in treating of advanced lung cancer.
Keywords: chemotherapy; drug sensitivity test; lung cancer; patient-derived organoid; personalized medicine; real-world study; targeted therapy.
Copyright © 2022 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The authors declare no competing interests.
Figures
Comment in
-
Moving toward precision medicine with lung cancer organoids.Cell Rep Med. 2023 Feb 21;4(2):100952. doi: 10.1016/j.xcrm.2023.100952. Cell Rep Med. 2023. PMID: 36812886 Free PMC article.
References
-
- Pauli C., Hopkins B.D., Prandi D., Shaw R., Fedrizzi T., Sboner A., Sailer V., Augello M., Puca L., Rosati R., et al. Personalized in vitro and in vivo cancer models to guide precision medicine. Cancer Discov. 2017;7:462–477. doi: 10.1158/2159-8290.CD-16-1154. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
