

Physical Activity, Sedentary Behavior, and Risk of Coronavirus Disease 2019
- PMID: 36657558
- PMCID: PMC9842390
- DOI: 10.1016/j.amjmed.2022.12.029
Physical Activity, Sedentary Behavior, and Risk of Coronavirus Disease 2019
Abstract
Introduction: Data on the associations of prepandemic physical activity and sedentary behavior with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and coronavirus disease 2019 (COVID-19) severity, particularly milder illness, have been limited.
Methods: We used data from 43,913 participants within the Nurses' Health Study II and Health Professionals Follow-Up Study who responded to periodic COVID-related surveys from May 2020 through March 2021. History of physical activity from the prepandemic period was assessed as the metabolic equivalents of task (MET)-hours per week of various activities of different intensity and sedentary behavior assessed from reports of time spent sitting from questionnaires completed 2016-2017. Multivariable logistic regression models were fitted to calculate the odds ratios (ORs) and 95% confidence intervals (CIs) for risk of SARS-CoV-2 infection and COVID-19 severity, as well as predicted COVID-19 defined using a validated symptom-based algorithm.
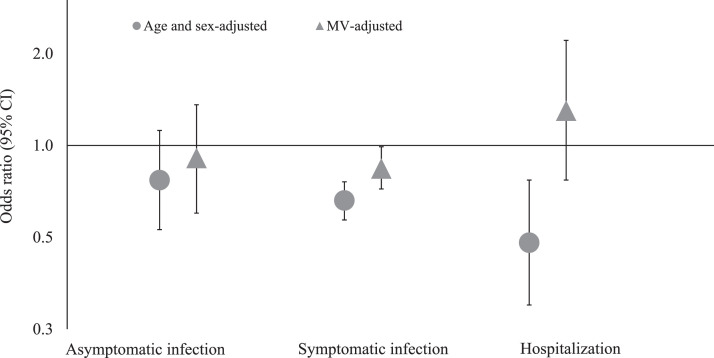
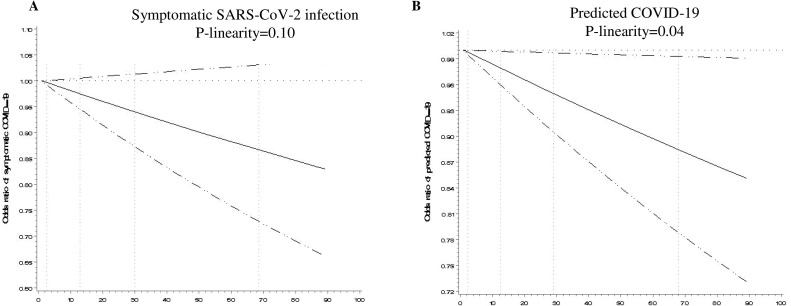
Results: Higher levels of prepandemic physical activity were associated with a lower risk for SARS-CoV-2 infection. Compared to participants with <3 MET-hours per week, the multivariable-adjusted OR was 0.86 (95% CI: 0.74, 0.99; P trend =.07) for those with ≥27 MET-hours per week. Higher physical activity levels were also associated with lower risk of symptomatic SARS-CoV-2 infection (OR: 0.84; 95% CI: 0.72, 0.99; P trend = .05) and predicted COVID-19 (OR: 0.87; 95% CI: 0.78, 0.97; P trend = .01). Longer time sitting at home watching TV (OR: 0.85; 95% CI: 0.73, 0.97) or for other tasks (OR: 0.78; 95% CI: 0.66, 0.92) was associated with a lower risk of SARS-CoV-2 infection.
Conclusions: Our findings support a protective association between prepandemic physical activity and lower risk and severity of COVID-19.
Keywords: COVID-19; Physical activity; SARS-CoV-2 infection; Sedentary behavior.
Copyright © 2023 Elsevier Inc. All rights reserved.
Figures

Comment in
-
Using SARS-CoV-2 Antibody Testing in COVID-19 Research.Am J Med. 2023 Jun;136(6):501-503. doi: 10.1016/j.amjmed.2023.02.001. Epub 2023 Feb 12. Am J Med. 2023. PMID: 36780969 Free PMC article. No abstract available.
References
-
- World Health Organization (WHO). WHO Coronavirus (COVID-19) Dashboard. https://covid19.who.int/. Accessed March 1, 2022.
-
- Haas EJ, Angulo FJ, McLaughlin JM, et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: an observational study using national surveillance data. Lancet. 2021;397:1819–1829. - PMC - PubMed
-
- Centers for Disease Control and Prevention. https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/index.html. Accessed March 1, 2022.
-
- Myers J. Cardiology patient pages. Exercise and cardiovascular health. Circulation. 2003;107:e2–e5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
