

Novel EGFR-mutant mouse models of lung adenocarcinoma reveal adaptive immunity requirement for durable osimertinib response
- PMID: 36657561
- PMCID: PMC10544803
- DOI: 10.1016/j.canlet.2023.216062
Novel EGFR-mutant mouse models of lung adenocarcinoma reveal adaptive immunity requirement for durable osimertinib response
Abstract
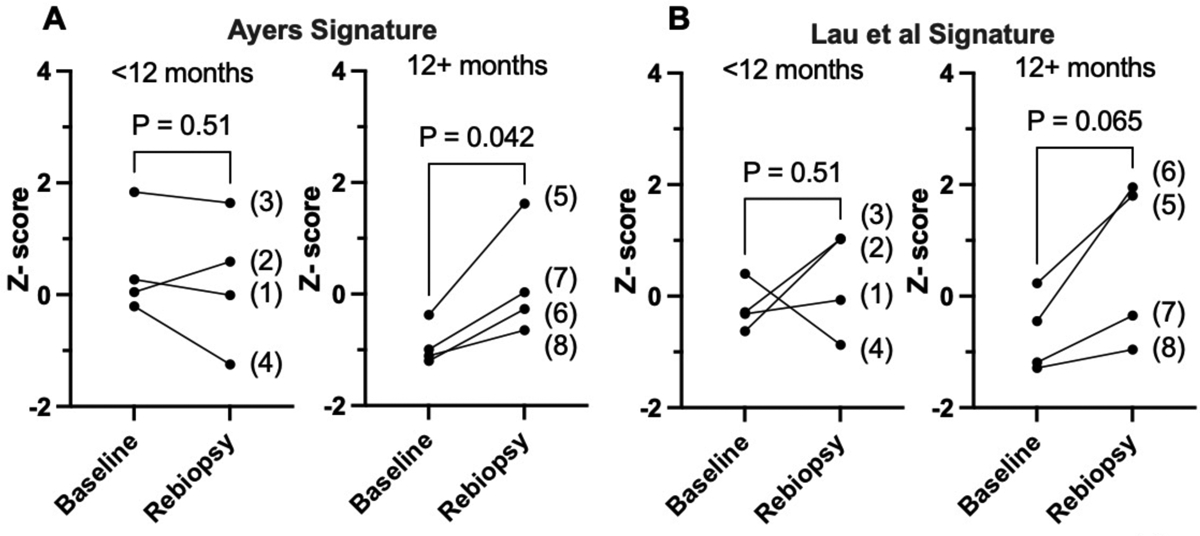
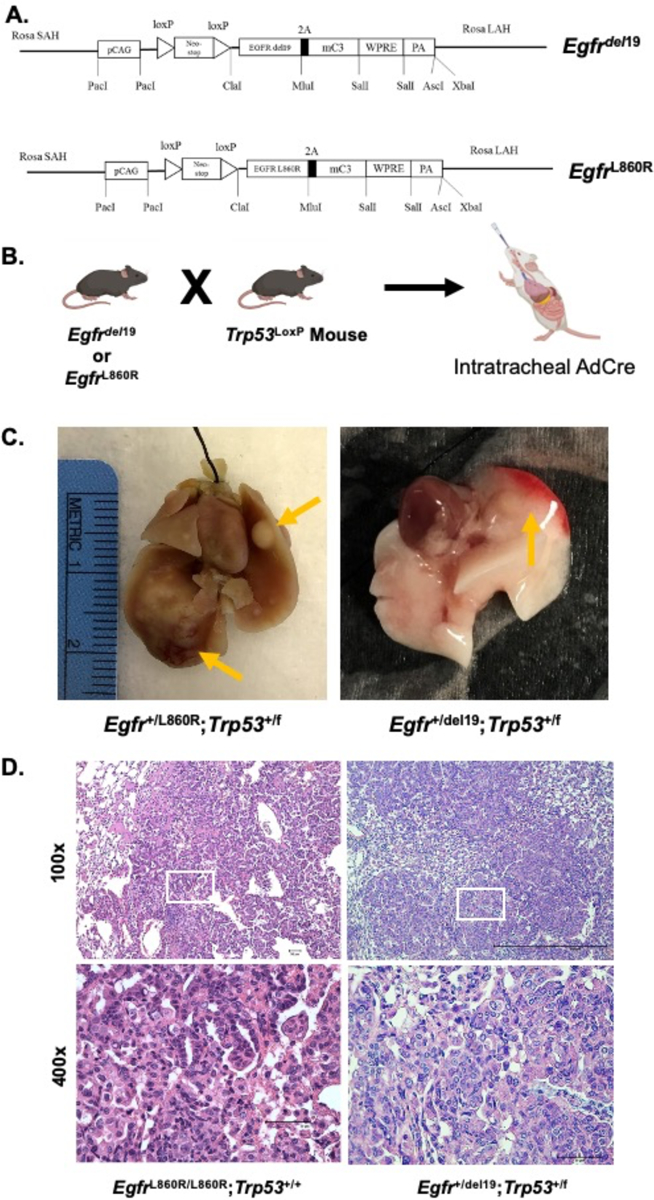
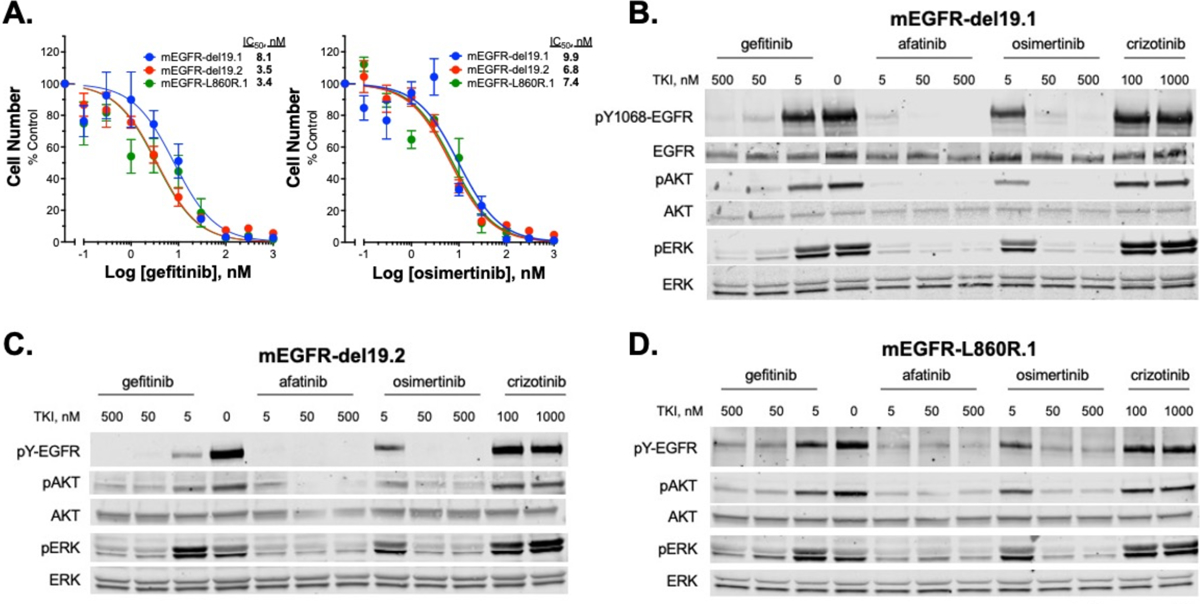
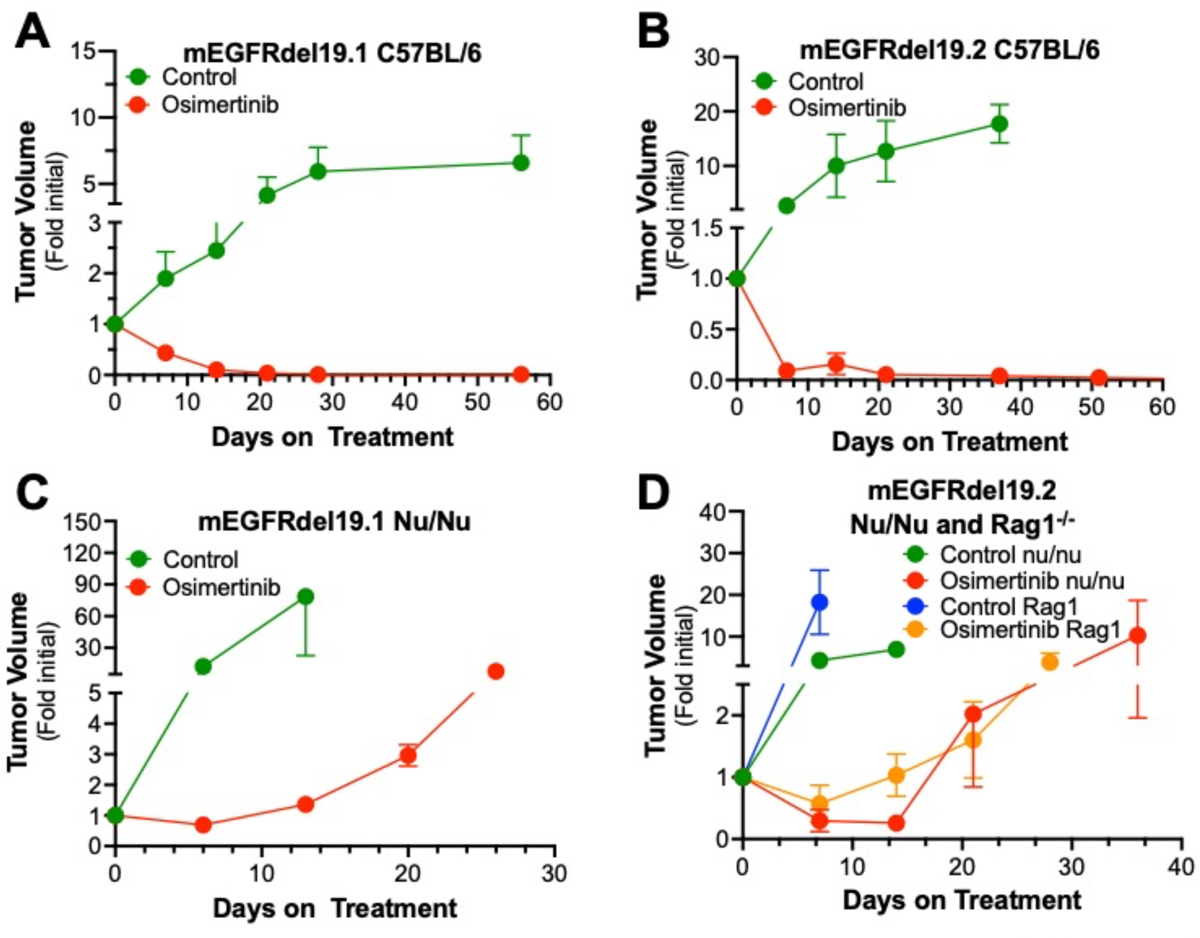
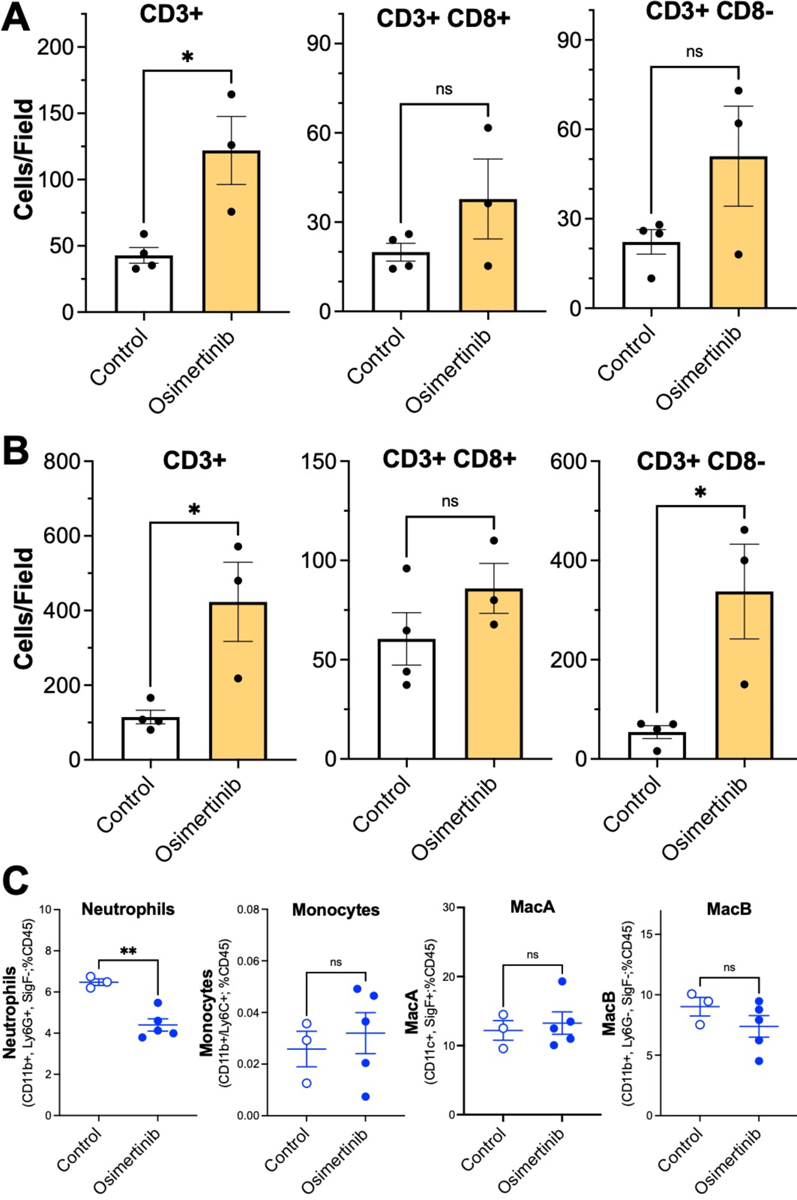
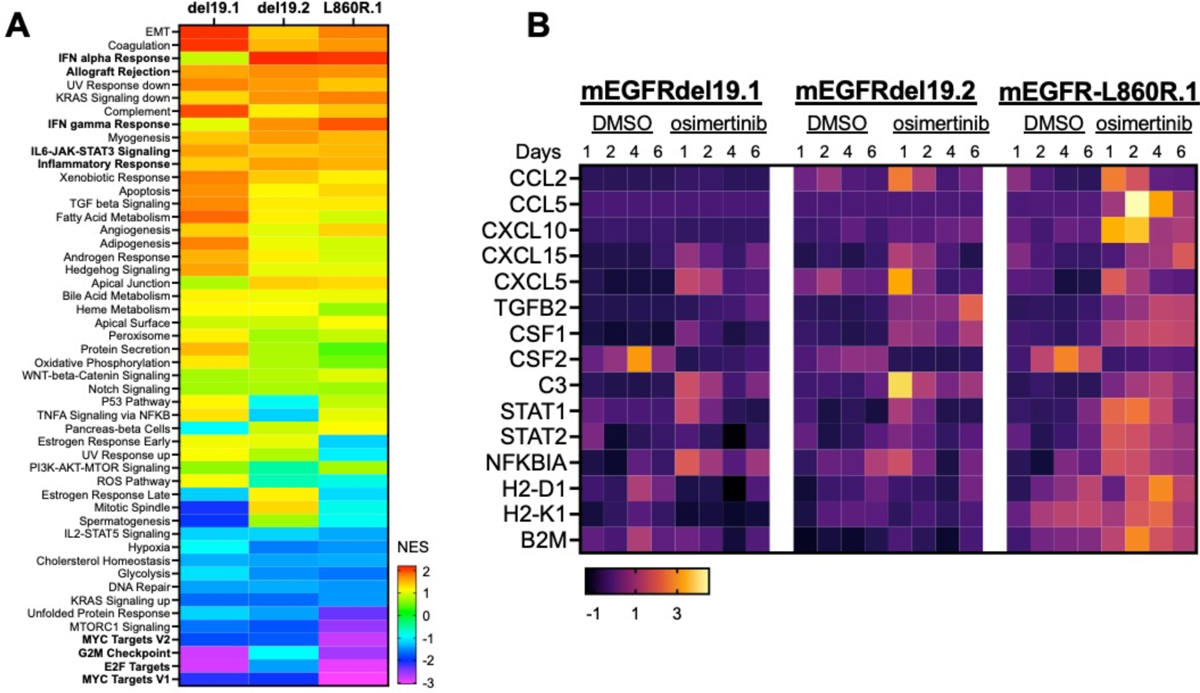
Lung cancers bearing oncogenically-mutated EGFR represent a significant fraction of lung adenocarcinomas (LUADs) for which EGFR-targeting tyrosine kinase inhibitors (TKIs) provide a highly effective therapeutic approach. However, these lung cancers eventually acquire resistance and undergo progression within a characteristically broad treatment duration range. Our previous study of EGFR mutant lung cancer patient biopsies highlighted the positive association of a TKI-induced interferon γ transcriptional response with increased time to treatment progression. To test the hypothesis that host immunity contributes to the TKI response, we developed novel genetically-engineered mouse models of EGFR mutant lung cancer bearing exon 19 deletions (del19) or the L860R missense mutation. Both oncogenic EGFR mouse models developed multifocal LUADs from which transplantable cancer cell lines sensitive to the EGFR-specific TKIs, gefitinib and osimertinib, were derived. When propagated orthotopically in the left lungs of syngeneic C57BL/6 mice, deep and durable shrinkage of the cell line-derived tumors was observed in response to daily treatment with osimertinib. By contrast, orthotopic tumors propagated in immune deficient nu/nu or Rag1-/- mice exhibited modest tumor shrinkage followed by rapid progression on continuous osimertinib treatment. Importantly, osimertinib treatment significantly increased intratumoral T cell content and decreased neutrophil content relative to diluent treatment. The findings provide strong evidence supporting the requirement for adaptive immunity in the durable therapeutic control of EGFR mutant lung cancer.
Keywords: Adaptive immunity; EGFR; GEMM; Lung adenocarcinoma; Tyrosine kinase inhibitor.
Copyright © 2023. Published by Elsevier B.V.
Conflict of interest statement
Declaration of competing interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Graham RP, Treece AL, Lindeman NI, Vasalos P, Shan M, Jennings LJ, Rimm DL, Worldwide Frequency of Commonly Detected EGFR Mutations, Arch Pathol Lab Med, 142 (2018) 163–167. - PubMed
-
- Cohen MH, Johnson JR, Chen YF, Sridhara R, Pazdur R, FDA drug approval summary: erlotinib (Tarceva) tablets, Oncologist, 10 (2005) 461–466. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
