

Liquid biopsy approaches to capture tumor evolution and clinical outcomes during cancer immunotherapy
- PMID: 36657818
- PMCID: PMC9853269
- DOI: 10.1136/jitc-2022-005924
Liquid biopsy approaches to capture tumor evolution and clinical outcomes during cancer immunotherapy
Abstract
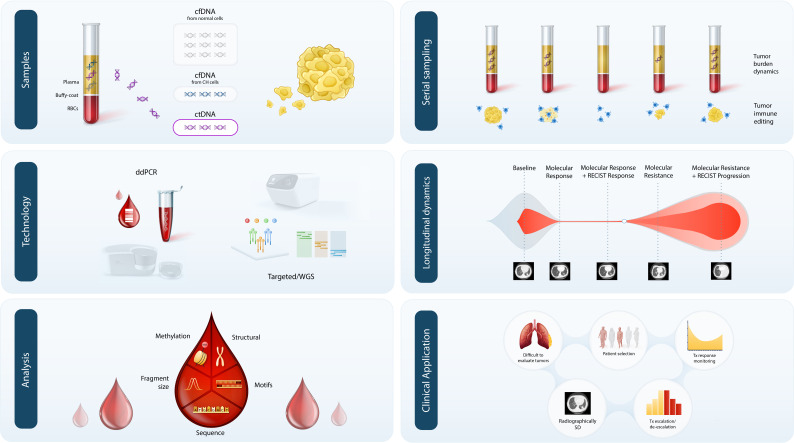
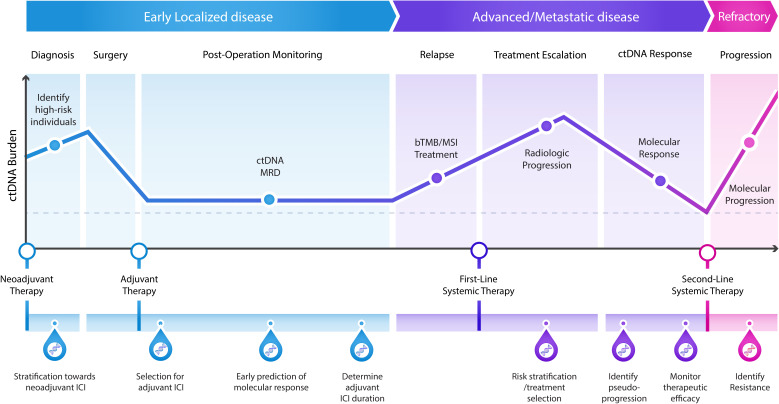
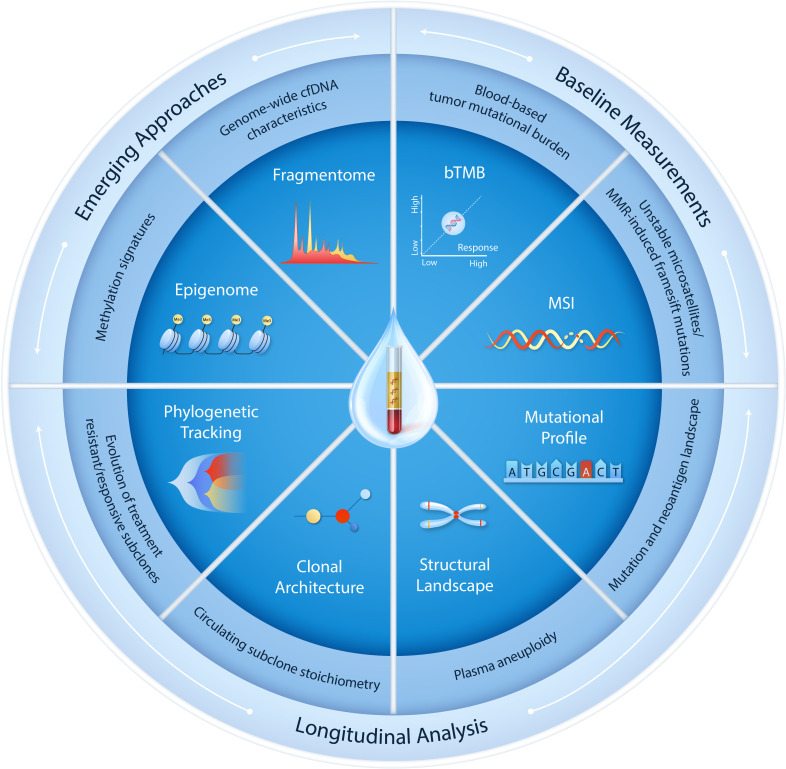
Circulating cell-free tumor DNA (ctDNA) can serve as a real-time biomarker of tumor burden and provide unique insights into the evolving molecular landscape of cancers under the selective pressure of immunotherapy. Tracking the landscape of genomic alterations detected in ctDNA may reveal the clonal architecture of the metastatic cascade and thus improve our understanding of the molecular wiring of therapeutic responses. While liquid biopsies may provide a rapid and accurate evaluation of tumor burden dynamics during immunotherapy, the complexity of antitumor immune responses is not fully captured through single-feature ctDNA analyses. This underscores a need for integrative studies modeling the tumor and the immune compartment to understand the kinetics of tumor clearance in association with the quality of antitumor immune responses. Clinical applications of ctDNA testing in patients treated with immune checkpoint inhibitors have shown both predictive and prognostic value through the detection of genomic biomarkers, such as tumor mutational burden and microsatellite instability, as well as allowing for real-time monitoring of circulating tumor burden and the assessment of early on-therapy responses. These efforts highlight the emerging role of liquid biopsies in selecting patients for cancer immunotherapy, monitoring therapeutic efficacy, determining the optimal duration of treatment and ultimately guiding treatment selection and sequencing. The clinical translation of liquid biopsies is propelled by the increasing number of ctDNA-directed interventional clinical trials in the immuno-oncology space, signifying a critical step towards implementation of liquid biopsies in precision immuno-oncology.
Keywords: Genetic Markers; Immunotherapy; Tumor Biomarkers.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: VA receives research funding to Johns Hopkins University from Astra Zeneca, Personal Genome Diagnostics and Delfi Diagnostics and has received research funding to Johns Hopkins University from Bristol-Myers Squibb in the past 5 years. VA is an inventor on patent applications (63/276,525, 17/779,936, 16/312,152, 16/341,862, 17/047,006 and 17/598,690) submitted by Johns Hopkins University related to cancer genomic analyses, ctDNA therapeutic response monitoring and immunogenomic features of response to immunotherapy that have been licensed to one or more entities. Under the terms of these license agreements, the University and inventors are entitled to fees and royalty distributions. JVC has served on an advisory board for Illumina. JCM has served in a consulting role to MJH Life Sciences, Johnson & Johnson, and Doximity and has received research funding to his institution from Merck via the Conquer Cancer Young Investigators Award. BPL has served in a consultant/advisory role for Janssen, Daiichi Sankyo, AstraZeneca, Eli Lilly, Genentech, Mirati, Amgen, Pfizer, BMS, Guardant 360, and Foundation Medicine. SS has served in a consultant/advisory role for Genentech and MJH Life Sciences. VL has served in a consultant/advisory role for Takeda, Seattle Genetics, Bristol-Myers Squibb, AstraZeneca and Guardant Health and has received research funding from GlaxoSmithKline, BMS, Merck and Seattle Genetics. MS and JJ are employees of Personal Genome Diagnostics (Labcorp).
Figures
Comment in
-
Next-generation ctDNA-driven clinical trials in precision immuno-oncology.J Immunother Cancer. 2023 Jan;11(1):e006397. doi: 10.1136/jitc-2022-006397. J Immunother Cancer. 2023. PMID: 36657816 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical