

CAR-T Cell-Mediated B-Cell Depletion in Central Nervous System Autoimmunity
- PMID: 36657993
- PMCID: PMC9853314
- DOI: 10.1212/NXI.0000000000200080
CAR-T Cell-Mediated B-Cell Depletion in Central Nervous System Autoimmunity
Abstract
Background and objectives: Anti-CD20 monoclonal antibody (mAb) B-cell depletion is a remarkably successful multiple sclerosis (MS) treatment. Chimeric antigen receptor (CAR)-T cells, which target antigens in a non-major histocompatibility complex (MHC)-restricted manner, can penetrate tissues more thoroughly than mAbs. However, a previous study indicated that anti-CD19 CAR-T cells can paradoxically exacerbate experimental autoimmune encephalomyelitis (EAE) disease. We tested anti-CD19 CAR-T cells in a B-cell-dependent EAE model that is responsive to anti-CD20 B-cell depletion similar to the clinical benefit of anti-CD20 mAb treatment in MS.
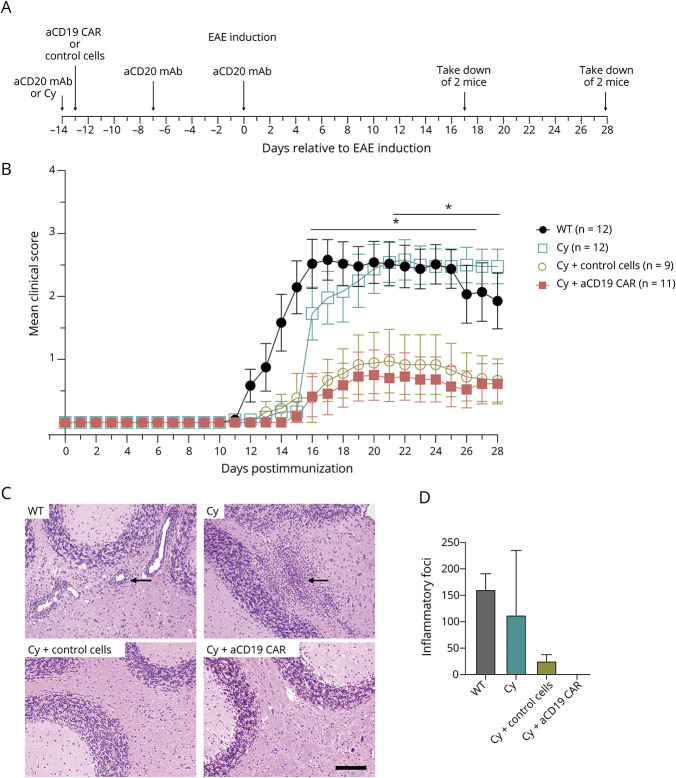
Methods: Anti-CD19 CAR-T cells or control cells that overexpressed green fluorescent protein were transferred into C57BL/6 mice pretreated with cyclophosphamide (Cy). Mice were immunized with recombinant human (rh) myelin oligodendrocyte protein (MOG), which causes EAE in a B-cell-dependent manner. Mice were evaluated for B-cell depletion, clinical and histologic signs of EAE, and immune modulation.
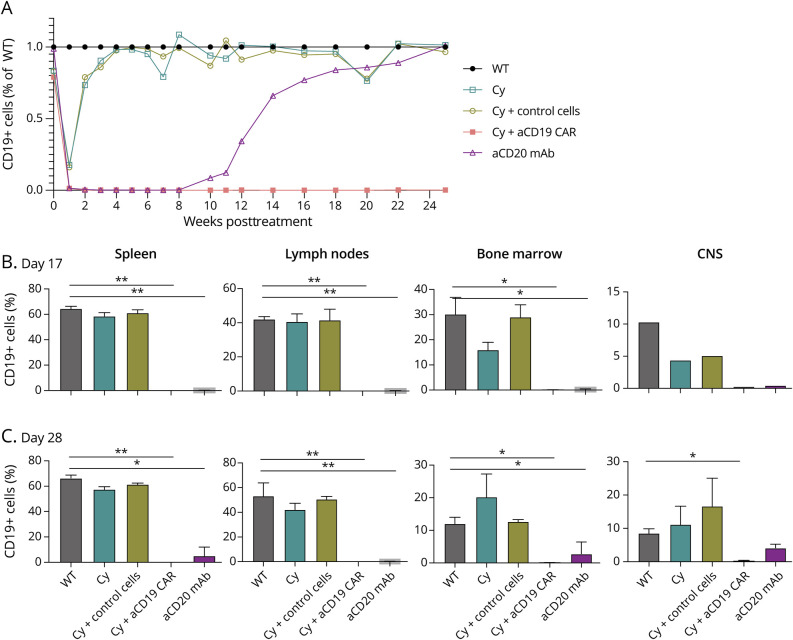
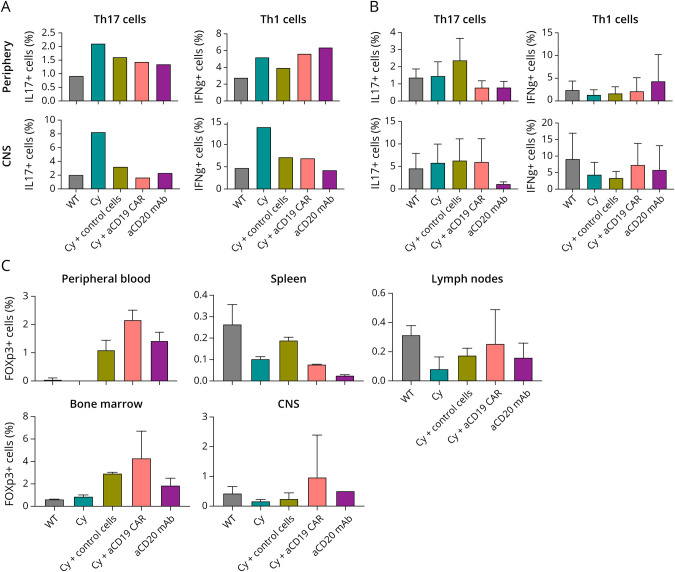
Results: Clinical scores and lymphocyte infiltration were reduced in mice treated with either anti-CD19 CAR-T cells with Cy or control cells with Cy, but not with Cy alone. B-cell depletion was observed in peripheral lymphoid tissue and in the CNS of mice treated with anti-CD19 CAR-T cells with Cy pretreatment. Th1 or Th17 populations did not differ in anti-CD19 CAR-T cell, control cell-treated animals, or Cy alone.
Discussion: In contrast to previous data showing that anti-CD19 CAR-T cell treatment exacerbated EAE, we observed that anti-CD19 CAR-T cells ameliorated EAE. In addition, anti-CD19 CAR-T cells thoroughly depleted B cells in peripheral tissues and in the CNS. However, the clinical benefit occurred independently of antigen specificity or B-cell depletion.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials