

Principal component analysis of flow-volume curves in COPDGene to link spirometry with phenotypes of COPD
- PMID: 36658542
- PMCID: PMC9854102
- DOI: 10.1186/s12931-023-02318-4
Principal component analysis of flow-volume curves in COPDGene to link spirometry with phenotypes of COPD
Abstract
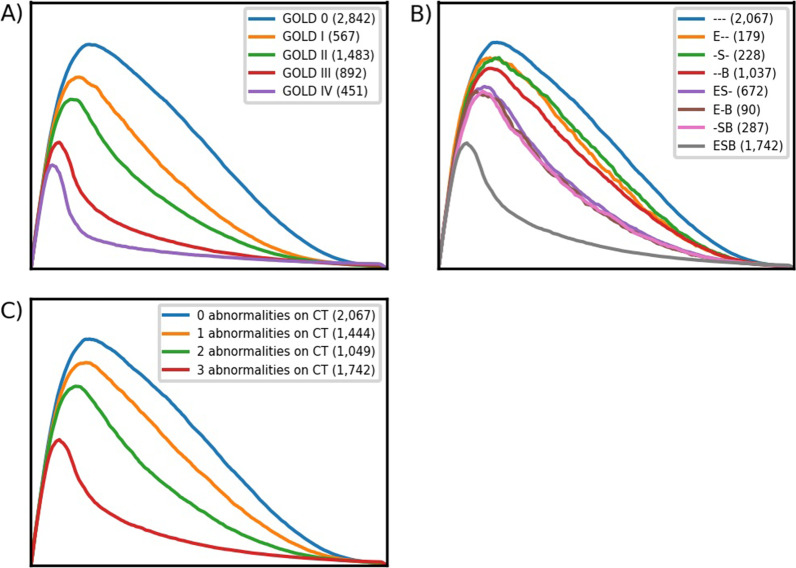
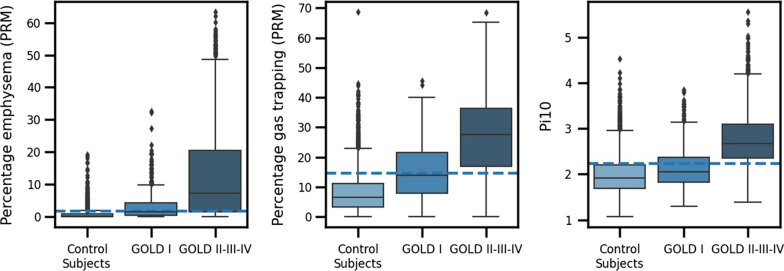
Background: Parameters from maximal expiratory flow-volume curves (MEFVC) have been linked to CT-based parameters of COPD. However, the association between MEFVC shape and phenotypes like emphysema, small airways disease (SAD) and bronchial wall thickening (BWT) has not been investigated.
Research question: We analyzed if the shape of MEFVC can be linked to CT-determined emphysema, SAD and BWT in a large cohort of COPDGene participants.
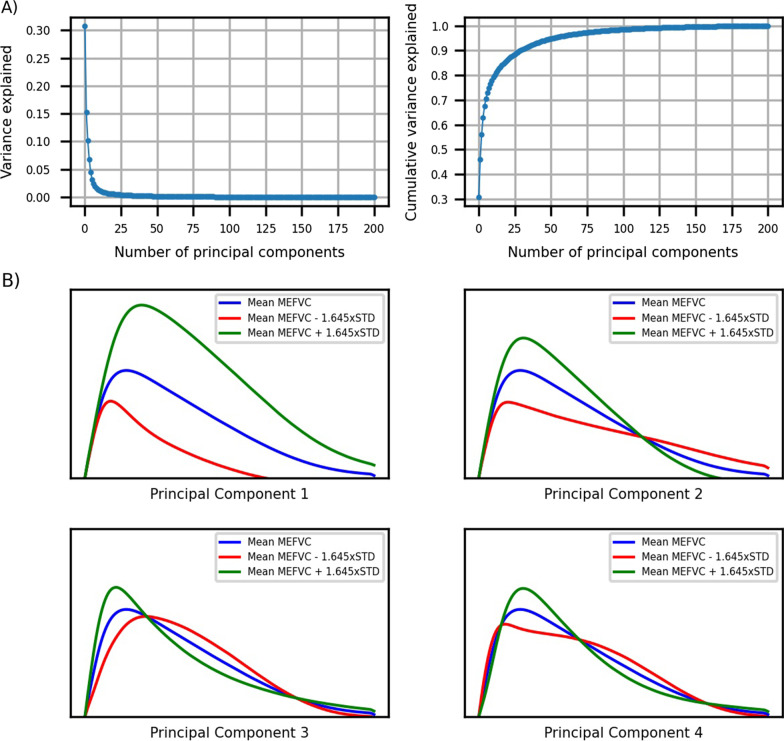
Study design and methods: In the COPDGene cohort, we used principal component analysis (PCA) to extract patterns from MEFVC shape and performed multiple linear regression to assess the association of these patterns with CT parameters over the COPD spectrum, in mild and moderate-severe COPD.
Results: Over the entire spectrum, in mild and moderate-severe COPD, principal components of MEFVC were important predictors for the continuous CT parameters. Their contribution to the prediction of emphysema diminished when classical pulmonary function test parameters were added. For SAD, the components remained very strong predictors. The adjusted R2 was higher in moderate-severe COPD, while in mild COPD, the adjusted R2 for all CT outcomes was low; 0.28 for emphysema, 0.21 for SAD and 0.19 for BWT.
Interpretation: The shape of the maximal expiratory flow-volume curve as analyzed with PCA is not an appropriate screening tool for early disease phenotypes identified by CT scan. However, it contributes to assessing emphysema and SAD in moderate-severe COPD.
Keywords: COPD; Computed tomography; Maximal expiratory flow-volume curve; Principal component analysis.
© 2023. The Author(s).
Conflict of interest statement
KV has nothing to disclose. ND has nothing to disclose. IG receives personal funding from Research Foundation Flanders (FWO). MT is CEO and co-founder of ArtiQ but received no payments related to the manuscript. TT has nothing to disclose. JDC received funding from NIH Grant Support R01-089897 and is chairman of the COPD Foundation Board of Directors. EKS received funding from NIH Grant Support and institutional grant support from GlaxoSmithKline and Bayer. BJM received funding from NHLBI, grants from AstraZeneca, GlaxoSmithKline and Pearl Research and fees from AstraZeneca, GlaxoSmithKline, Sunovion, Verona, Boehringer Ingelheim, Takeda, Third Pole, Phillips and Circasia. He is member of the NHLBI and Spiration Data Safety Monitoring Boards and chairman of Mt. Sinai SOM Data Safety Monitoring Board. ER received a COPDGene grant from NHBLI. RJ received consulting fees from National Jewish Health for an LLC he owns. MDV received funding from the AI in Flanders project. WJ received grants from AstraZeneca and Chiesi and obtained fees from AstraZeneca, Chiesi and GlaxoSmithKline. He is chairman of Board of Flemish Society for TBC prevention and board member of ArtiQ.
Figures
Similar articles
-
Validation of a method to assess emphysema severity by spirometry in the COPDGene study.Respir Res. 2020 May 1;21(1):103. doi: 10.1186/s12931-020-01366-4. Respir Res. 2020. PMID: 32357885 Free PMC article.
-
Five-year Progression of Emphysema and Air Trapping at CT in Smokers with and Those without Chronic Obstructive Pulmonary Disease: Results from the COPDGene Study.Radiology. 2020 Apr;295(1):218-226. doi: 10.1148/radiol.2020191429. Epub 2020 Feb 4. Radiology. 2020. PMID: 32013794 Free PMC article.
-
Phenotype of Spirometric Impairment in an Aging Population.Am J Respir Crit Care Med. 2016 Apr 1;193(7):727-35. doi: 10.1164/rccm.201508-1603OC. Am J Respir Crit Care Med. 2016. PMID: 26540012 Free PMC article.
-
Future Perspectives of Revaluating Mild COPD.Respiration. 2022;101(7):688-696. doi: 10.1159/000524102. Epub 2022 Apr 25. Respiration. 2022. PMID: 35468602 Review.
-
Quantitative computed tomography measurements to evaluate airway disease in chronic obstructive pulmonary disease: Relationship to physiological measurements, clinical index and visual assessment of airway disease.Eur J Radiol. 2016 Nov;85(11):2144-2151. doi: 10.1016/j.ejrad.2016.09.010. Epub 2016 Sep 13. Eur J Radiol. 2016. PMID: 27776670 Free PMC article. Review.
Cited by
-
Consequences of Preterm Birth: Knowns, Unknowns, and Barriers to Advancing Cardiopulmonary Health.Integr Comp Biol. 2023 Sep 15;63(3):693-704. doi: 10.1093/icb/icad045. Integr Comp Biol. 2023. PMID: 37253617 Free PMC article.
References
-
- Vestbo J, Anderson JA, Brook RD, et al. Fluticasone furoate and vilanterol and survival in chronic obstructive pulmonary disease with heightened cardiovascular risk (SUMMIT): A double-blind randomised controlled trial. Lancet. 2016;387(10030):1817–1826. doi: 10.1016/S0140-6736(16)30069-1. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
