

Inter- and intra-observer agreement in the assessment of the cervical transformation zone (TZ) by visual inspection with acetic acid (VIA) and its implications for a screen and treat approach: a reliability study
- PMID: 36658551
- PMCID: PMC9854065
- DOI: 10.1186/s12905-022-02131-z
Inter- and intra-observer agreement in the assessment of the cervical transformation zone (TZ) by visual inspection with acetic acid (VIA) and its implications for a screen and treat approach: a reliability study
Abstract
Background: In low-resource countries, interpretation of the transformation zone (TZ) using the classification of the International Federation for Cervical Pathology and Colposcopy (IFCPC), adopted by the World Health Organization, is critical for determining if visual inspection with acetic acid (VIA) screening and thermal ablation treatment are possible. We aim to assess inter- and intra-observer agreement in TZ interpretation.
Methods: We performed a prospective multi-observer reliability study. One hundred cervical digital images of Human papillomavirus positive women (30-49 years) were consecutively selected from a Cameroonian cervical cancer screening trial. Images of the native cervix and after VIA were obtained. The images were evaluated for the TZ type at two time points (rounds one and two) by five VIA experts from four countries (Côte d'Ivoire, Cameroon, Peru, and Zambia) according to the IFCPC classification (TZ1 = ectocervical fully visible; TZ2 = endocervical fully visible; TZ3 = not fully visible). Intra- and inter-observer agreement were measured by Fleiss' kappa.
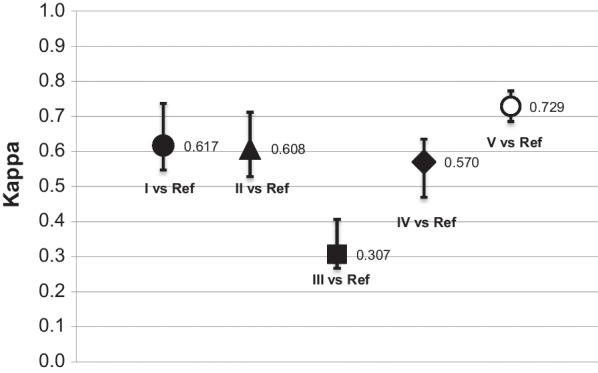
Results: Overall, 37.0% of images were interpreted as TZ1, 36.4% as TZ2, and 26.6% as TZ3. Global inter-observer reliability indicated fair agreement in both rounds (kappa 0.313 and 0.288). The inter-observer agreement was moderate for TZ1 interpretation (0.460), slight for TZ2 (0.153), and fair for TZ3 (0.329). Intra-observer analysis showed fair agreement for two observers (0.356 and 0.345), moderate agreement for two other (0.562 and 0.549), and one with substantial agreement (0.728).
Conclusion: Interpretation of the TZ using the IFCPC classification, adopted by the World Health Organization, is critical for determining if VIA screening and thermal ablation treatment are possible. However, the low inter- and intra-observer agreement suggest that the reliability of the referred classification is limited in the context of VIA. It's integration in treatment recommendations should be used with caution since TZ3 interpretation could lead to an important referral rate for further evaluation. Trial registration Cantonal Ethics Board of Geneva, Switzerland: N°2017-0110. Cameroonian National Ethics Committee for Human Health Research N°2018/07/1083/CE/CNERSH/SP.
Keywords: Agreement; Cervical cancer; International Federation for Cervical Pathology and Colposcopy; Kappa; Low-resource setting; Reliability; Transformation zone type; Visual inspection with acetic acid.
© 2023. The Author(s).
Conflict of interest statement
All authors have no conflicts of interest.
Figures
References
-
- World Health Organization. WHO guidelines for the use of thermal ablation for cervical pre-cancer lesions. 2019. Available from: https://apps.who.int/iris/bitstream/handle/10665/329299/9789241550598-en.... Accessed 09 Feb 2021. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
