

Management of Helicobacter pylori infection
- PMID: 36660052
- PMCID: PMC9840198
- DOI: 10.1002/jgh3.12843
Management of Helicobacter pylori infection
Abstract
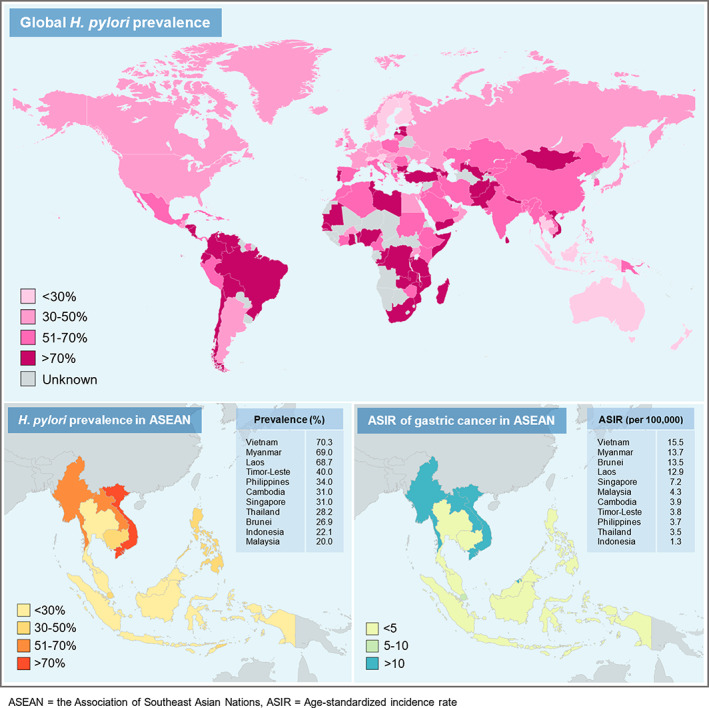
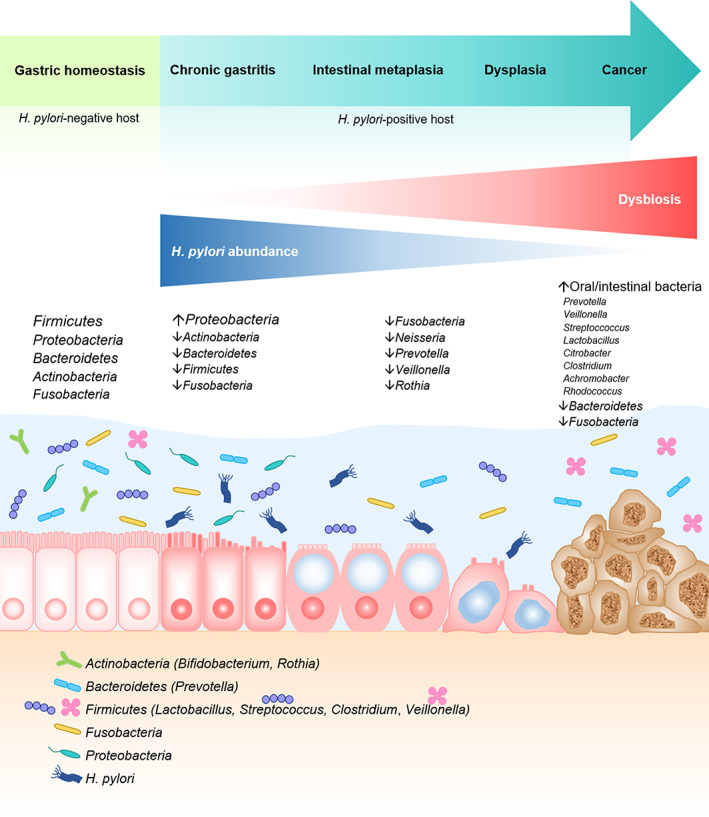
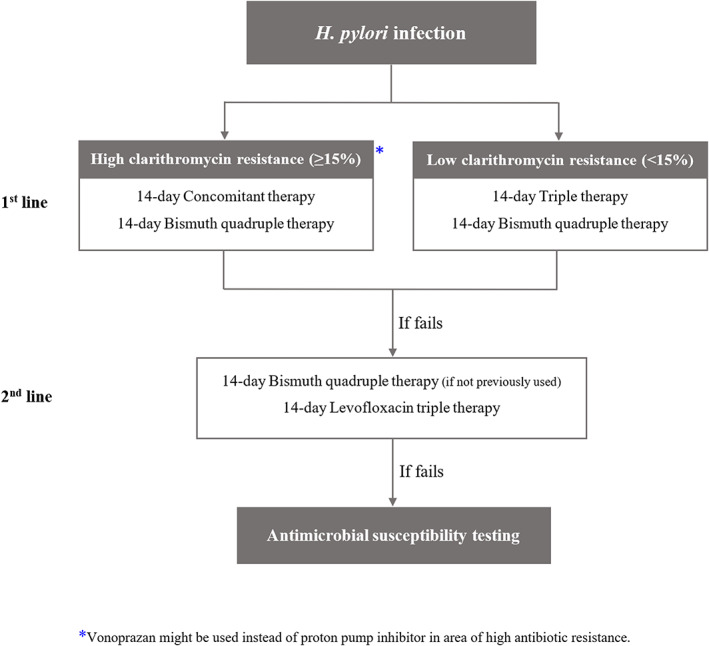
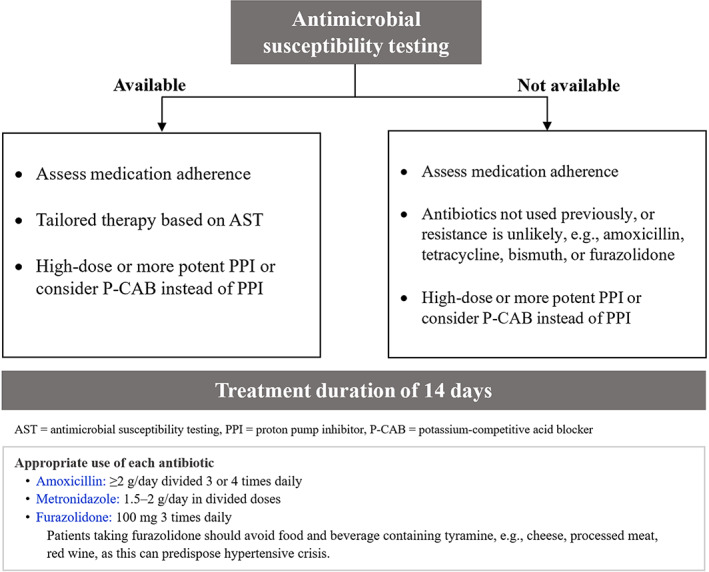
Helicobacter pylori infection exhibits a wide disease spectrum ranging from asymptomatic gastritis, peptic ulcer disease, to gastric cancer. H. pylori can induce dysbiosis of gastric microbiota in the pathway of carcinogenesis and successful eradication can restore gastric homeostasis. Diagnostic testing and treatment for H. pylori infection is recommended in patients with active or past history of peptic ulcer, chronic dyspepsia, chronic non-steroidal anti-inflammatory drugs (NSAID) or aspirin use, precancerous gastric lesions, gastric cancer, mucosa-associated lymphoid tissue (MALT) lymphoma, family history of gastric cancer, family history of peptic ulcers, household family member having active H. pylori infection, iron deficiency anemia, idiopathic thrombocytopenic purpura, or vitamin B12 deficiency. Recommended first-line regimens for H. pylori eradication are classified according to clarithromycin resistance. In areas of high clarithromycin resistance (≥15%), we recommend 14-day concomitant therapy or 14-day bismuth quadruple therapy (BQT) as first-line regimen. In areas of low clarithromycin resistance (<15%), we recommend 14-day triple therapy or 14-day BQT as first-line treatment. Second-line regimens are 14-day levofloxacin triple therapy or 14-day BQT if BQT is not previously used. For patients with multiple treatment failure, antimicrobial susceptibility testing (AST) should be performed. If AST is not available, we recommend using antibiotics not previously used or for which resistance is unlikely, such as amoxicillin, tetracycline, bismuth, or furazolidone. High-dose potent proton pump inhibitor or vonoprazan is recommended to achieve adequate acid suppression. Probiotics can be used as an adjuvant treatment to reduce the side effects of antibiotics and enhance eradication rate.
Keywords: Helicobacter pylori; management; treatment.
© 2022 The Authors. JGH Open published by Journal of Gastroenterology and Hepatology Foundation and John Wiley & Sons Australia, Ltd.
Figures
References
-
- Marshall BJ, Warren JR. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet. 1984; 1: 1311–15. - PubMed
-
- Sung H, Ferlay J, Siegel RL et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021; 71: 209–49. - PubMed
-
- Chey WD, Leontiadis GI, Howden CW, Moss SF. ACG Clinical Guideline: Treatment Of Helicobacter pylori Infection. Am. J. Gastroenterol. 2017; 112: 212–39. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
