

Intracranial Rosai-Dorfman Disease: A Case to Remember
- PMID: 36660540
- PMCID: PMC9845528
- DOI: 10.7759/cureus.32605
Intracranial Rosai-Dorfman Disease: A Case to Remember
Abstract
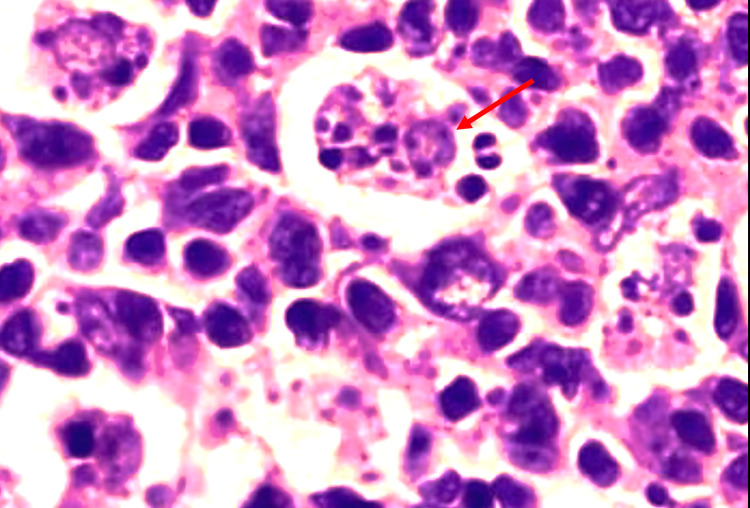
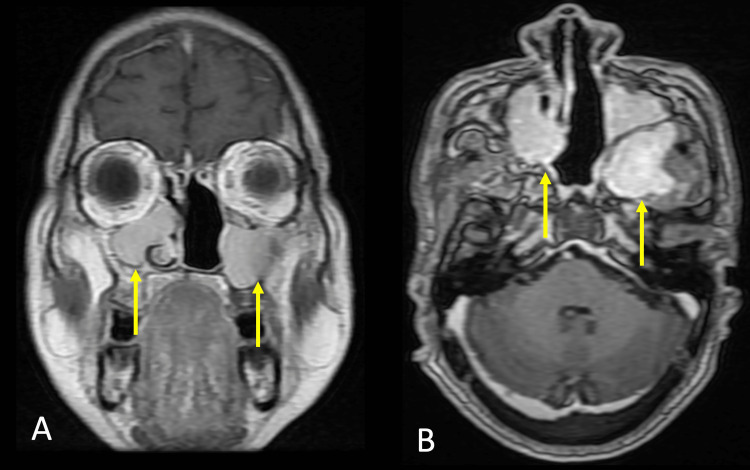
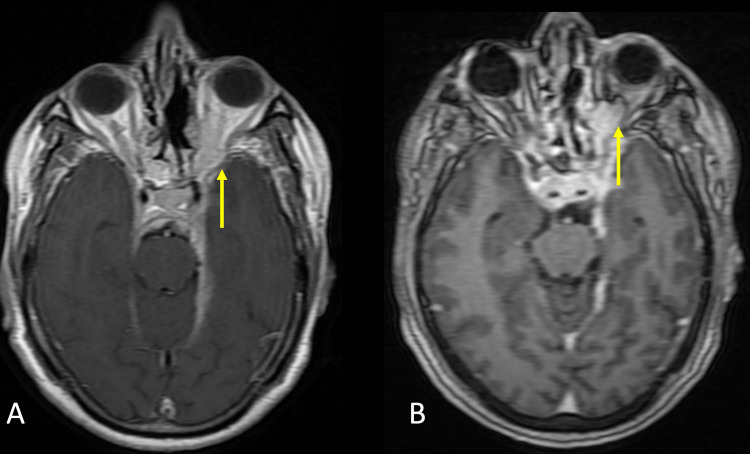
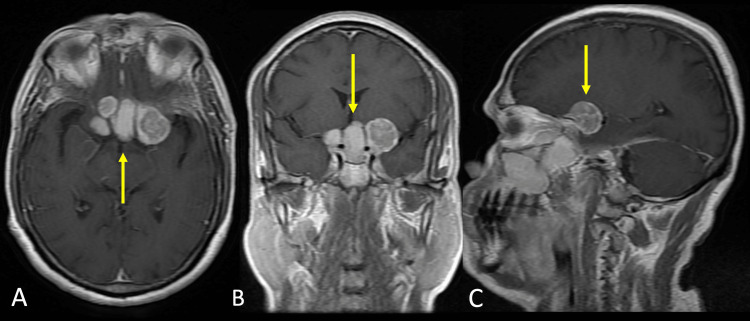
Sinus histiocytosis with massive lymphadenopathy (SHML), an alternative term for Rosai-Dorfman disease (RDD), is a rare benign idiopathic immune-related lymphoproliferative condition. The central nervous system (CNS) has been documented to be involved in RDD, although lymph nodes are the organs that are most frequently and primarily associated with the disease manifestation. Nonetheless, CNS involvement in RDD is rare and poorly understood. As a result, there is a lack of a solid basis for therapeutic approaches for CNS involvement in RDD. Here, we present a case of RDD with cerebral involvement, a rare presentation of RDD with atypical symptoms. A brief assessment of the radiographic appearance, histological findings, and the peculiar manifestations of the disease is provided.
Keywords: benign lymphoproliferative; hemophagocytic lympho-histiocytosis; intracranial neoplasms; neuro radiology; pet ct scan; rosai-dorfman disease; sinus histiocytosis with massive lymphadenopathy.
Copyright © 2022, Unadkat et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Adenitis with lipid excess, in children or young adults, seen in the Antilles and in Mali. (4 cases) (Article in French) Destombes P. https://pubmed.ncbi.nlm.nih.gov/5899730/ Bull Soc Pathol Exot Filiales. 1965;58:1169–1175. - PubMed
-
- Sinus histiocytosis with massive lymphadenopathy. A newly recognized benign clinicopathological entity. Rosai J, Dorfman RF. Arch Pathol. 1969;87:63–70. - PubMed
-
- FDG PET of Rosai-Dorfman disease of the thymus. Lim R, Wittram C, Ferry JA, Shepard JA. AJR Am J Roentgenol. 2004;182:514. - PubMed
-
- Rosai-Dorfman disease with primary cutaneous manifestations - a case report. Huang HY, Yang CL, Chen WJ. https://pubmed.ncbi.nlm.nih.gov/9791674/ Ann Acad Med Singap. 1998;27:589–593. - PubMed
-
- Cutaneous Rosai-Dorfman disease is a distinct clinical entity. Brenn T, Calonje E, Granter SR, Leonard N, Grayson W, Fletcher CD, McKee PH. Am J Dermatopathol. 2002;24:385–391. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials