

Efficacy and safety of percutaneous ultrasound-guided vacuum-assisted excision for the treatment of clinical benign breast lesions larger than 3 cm: a retrospective cohort study
- PMID: 36660716
- PMCID: PMC9843416
- DOI: 10.21037/atm-22-5829
Efficacy and safety of percutaneous ultrasound-guided vacuum-assisted excision for the treatment of clinical benign breast lesions larger than 3 cm: a retrospective cohort study
Abstract
Background: Breast ultrasound-guided vacuum-assisted excision (US-VAE) has become a scarless solution for the removal of benign breast lesions. This procedure is now favored by more and more female patients for its satisfactory cosmetic outcome and few postoperative complications. However, controversy have been raised regarding its efficacy and safety in treating larger benign breast lesions. This study aimed to evaluate whether US-VAE is sufficient for the treatment of clinical benign breast lesions larger than 3 cm and to investigate the lesion features that affect the complete excision rate and hematoma occurrence rate.
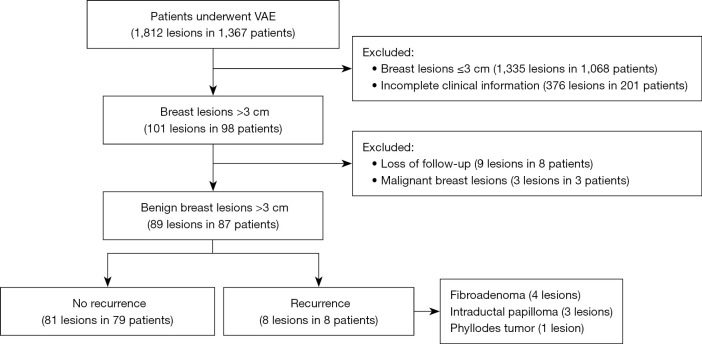
Methods: From January 2018 to July 2021, a total of 1,812 lesions in 1,367 patients underwent US-VAE at the Chinese People's Liberation Army General Hospital. A total of 89 benign breast lesions in 87 patients enrolled in this retrospective cohort study. The baseline clinical characteristics and ultrasonographic features of the lesions were recorded. Patients were followed up by US to record if there are any serious issues and the occurrence of hematoma and the recurrence of the lesions within 3 days and 6-12 months later, then at 1-year intervals. Lesions were classified to analyze the possible factors associated with complete excision rate and hematoma occurrence rate.
Results: The mean age was 35.9±9.5 years (range, 18-54 years), and the median maximum size of benign breast lesions was 3.5 cm (range, 3.1-5.0 cm). The complete excision rate was 91.0% (81/89). Histopathology (P=0.002) and vascularity (P=0.032) of lesions showed statistically significant differences in groups with or without recurrent lesions. A total of 17 cases (17/89, 19.1%) presented with hematoma after the procedure. The maximum lesion size in patients with hematoma was significantly larger than that in those without hematoma (P<0.001).
Conclusions: US-VAE is an effective and safe alternative method for the treatment of benign breast lesions larger than 3 cm, especially for fibroadenoma, adenosis, hamartoma. For benign phyllodes tumors and intraductal papillomas larger than 3 cm and lesions with hypervascularity, the possibility of recurrence after US-VAE should be noted. The size of lesions needs to be considered when evaluating the occurrence of hematoma after US-VAE.
Keywords: Ultrasound-guided vacuum-assisted excision (US-VAE); benign breast lesions; complete excision rate; hematoma occurrence rate.
2022 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://atm.amegroups.com/article/view/10.21037/atm-22-5829/coif). The authors have no conflicts of interest to declare.
Figures

References
LinkOut - more resources
Full Text Sources