

Racial and ethnic disparities in emergency department-initiated buprenorphine across five health care systems
- PMID: 36660800
- PMCID: PMC10467357
- DOI: 10.1111/acem.14668
Racial and ethnic disparities in emergency department-initiated buprenorphine across five health care systems
Abstract
Background: Opioid overdose deaths have disproportionately impacted Black and Hispanic populations, in part due to disparities in treatment access. Emergency departments (EDs) serve as a resource for patients with opioid use disorder (OUD), many of whom have difficulty accessing outpatient addiction programs. However, inequities in ED treatment for OUD remain poorly understood.
Methods: This secondary analysis examined racial and ethnic differences in buprenorphine access using data from EMBED, a study of 21 EDs across five health care systems evaluating a clinical decision support system for initiating ED buprenorphine. The primary outcome was receipt of buprenorphine, ED administered or prescribed. Hospital type (academic vs. community) was evaluated as an effect modifier. Hierarchical models with cluster effects for site and clinician were used to assess buprenorphine receipt by race and ethnicity.
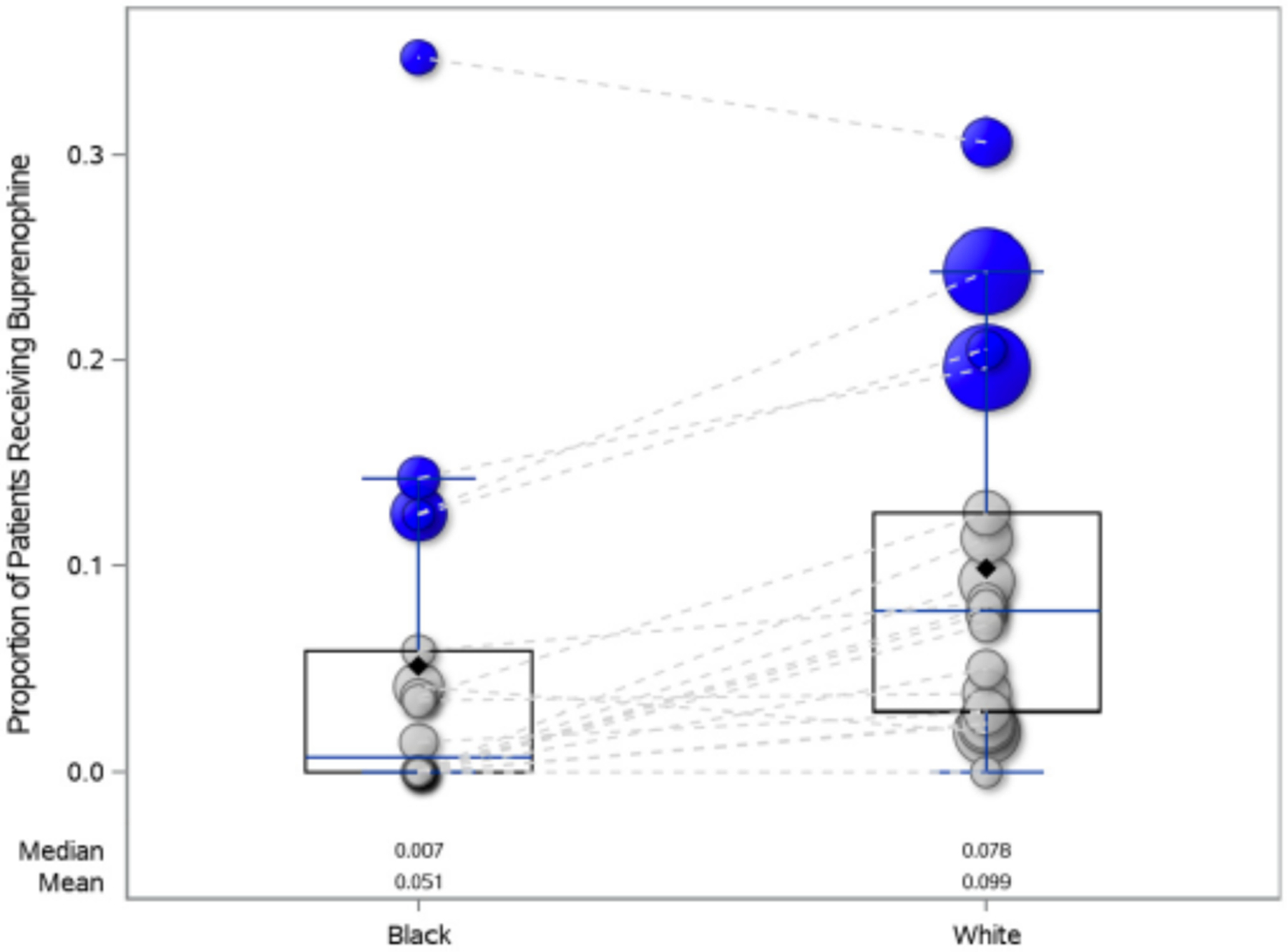
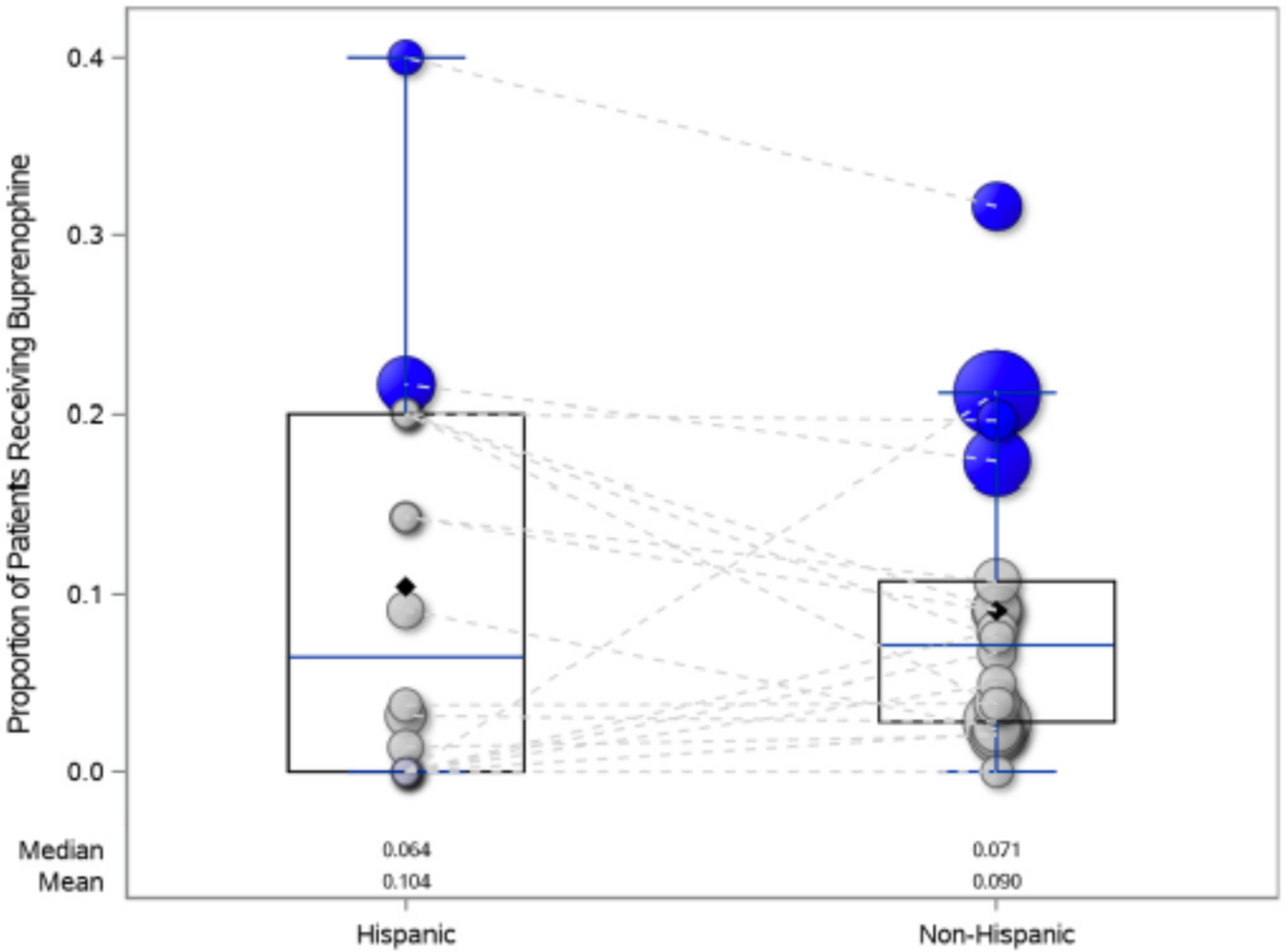
Results: Black patients were less likely to receive buprenorphine (6.4% [51/801] vs. White patients 8.5% [268/3154], odds ratio [OR] 0.59, 95% confidence interval [CI] 0.45-0.78). This association persisted after adjusting for age, insurance, gender, clinician X-waiver, hospital type, and urbanicity (adjusted OR [aOR] 0.64, 95% CI 0.48-0.84) but not when discharge diagnosis was included (aOR 0.75, 95% CI 0.56-1.02). Hispanic patients were more likely to receive buprenorphine (14.8% [122/822] vs. non-Hispanic patients, 11.6% [475/4098]) in unadjusted (OR 1.57, 95% CI 1.09-1.83) and adjusted models (aOR 1.41, 95% CI 1.08-1.83) but not including discharge diagnosis (aOR 1.32, 95% CI 0.99-1.77). Odds of buprenorphine were similar in academic and community EDs by race (interaction p = 0.97) and ethnicity (interaction p = 0.64).
Conclusions: Black patients with OUD were less likely to receive buprenorphine whereas Hispanic patients were more likely to receive buprenorphine in academic and community EDs. Differences were attenuated with discharge diagnosis, as fewer Black and non-Hispanic patients were diagnosed with opioid withdrawal. Barriers to medication treatment are heterogenous among patients with OUD; research must continue to address the multiple drivers of health inequities at the patient, clinician, and community level.
© 2023 The Authors. Academic Emergency Medicine published by Wiley Periodicals LLC on behalf of Society for Academic Emergency Medicine.
Conflict of interest statement
CONFLICT OF INTEREST STATEMENT
The authors declare no potential conflict of interest.
Figures
References
-
- Larochelle MR, Stopka TJ, Xuan Z, Liebschutz JM, Walley AY. Medication for opioid use disorder after nonfatal opioid overdose and mortality. Ann Intern Med. 2019;170(6):430–431. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
