

Long-Acting Cabotegravir and Rilpivirine Dosed Every 2 Months in Adults With Human Immunodeficiency Virus 1 Type 1 Infection: 152-Week Results From ATLAS-2M, a Randomized, Open-Label, Phase 3b, Noninferiority Study
- PMID: 36660819
- PMCID: PMC10156123
- DOI: 10.1093/cid/ciad020
Long-Acting Cabotegravir and Rilpivirine Dosed Every 2 Months in Adults With Human Immunodeficiency Virus 1 Type 1 Infection: 152-Week Results From ATLAS-2M, a Randomized, Open-Label, Phase 3b, Noninferiority Study
Abstract
Background: Cabotegravir (CAB) + rilpivirine (RPV) dosed intramuscularly monthly or every 2 months is a complete, long-acting (LA) regimen for the maintenance of HIV-1 virologic suppression. Here, we report the antiretroviral therapy as long acting suppression (ATLAS)-2M study week 152 results.
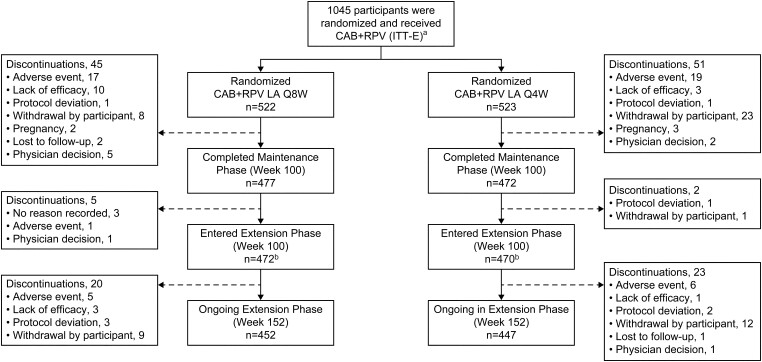
Methods: ATLAS-2M is a phase 3b, randomized, multicenter study assessing the efficacy and safety of CAB+RPV LA every 8 weeks (Q8W) versus every 4 weeks (Q4W). Virologically suppressed (HIV-1 RNA <50 copies/mL) individuals were randomized to receive CAB+RPV LA Q8W or Q4W. Endpoints included the proportion of participants with plasma HIV-1 RNA ≥50 copies/mL and <50 copies/mL, incidence of confirmed virologic failure (CVF; 2 consecutive measurements ≥200 copies/mL), safety, and tolerability.
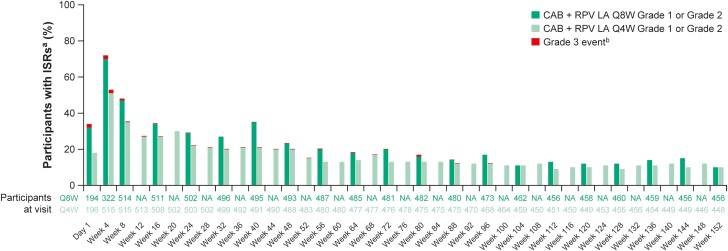
Results: A total of 1045 participants received CAB+RPV LA (Q8W, n = 522; Q4W, n = 523). CAB+RPV LA Q8W demonstrated noninferior efficacy versus Q4W dosing, with 2.7% (n = 14) and 1.0% (n = 5) of participants having HIV-1 RNA ≥50 copies/mL, respectively, with adjusted treatment difference being 1.7% (95% CI: 0.1-3.3%), meeting the 4% noninferiority threshold. At week 152, 87% of participants maintained HIV-1 RNA <50 copies/mL (Q8W, 87% [n = 456]; Q4W, 86% [n = 449]). Overall, 12 (2.3%) participants in the Q8W arm and 2 (0.4%) in the Q4W arm had CVF. Eight and 10 participants with CVF had treatment-emergent, resistance-associated mutations to RPV and integrase inhibitors, respectively. Safety profiles were comparable, with no new safety signals observed since week 48.
Conclusions: These data demonstrate virologic suppression durability with CAB+RPV LA Q8W or Q4W for ∼3 years and confirm long-term efficacy, safety, and tolerability of CAB+RPV LA as a complete regimen to maintain HIV-1 virologic suppression.
Keywords: HIV-1; antiretroviral therapy; cabotegravir; long-acting; rilpivirine.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. E. T. O. has received research support to their institution during the conduct of this study and has served as a consultant for Merck and ViiV Healthcare, outside of the submitted work. E. T. O. joined ViiV Healthcare after the conclusion of the week 152 analysis. G. Richmond received grants for clinical trials from Gilead, TaiMed, Insmed, and ViiV Healthcare, outside the submitted work. G. Rizzardini has received payment/honoraria from Gilead, GSK, MSD, and ViiV Healthcare, outside of the submitted work, and reports participation on a Data Safety Monitoring Board or Advisory Board for ViiV, GSK, and Gilead. A. T. has served as a consultant on advisory boards for GSK and received payment for presentations by GSK and ViiV Healthcare (Nordic countries), outside of the submitted work. S. N. reports consulting fees and payment or honoraria for lectures, presentations, speaker’s bureaus, manuscript writing, or education events from Gilead Sciences, MSD, Janssen, and ViiV Healthcare and support for attending meetings and/or travel from Gilead Sciences, Janssen, and ViiV Healthcare. N. P. reports payment of honoraria for educational events not related to this manuscript. A. W. reports grants and personal fees and honoraria for lectures and presentations from Gilead, Merck, and ViiV Healthcare, outside the submitted work. S. S. reports payments to their institution for clinical trial participation for the submitted work from ViiV Healthcare, salary support for research from the National Institutes of Health (NIH), and participation on a Data and Safety Monitoring Board for NIH. J. R. reports personal fees from Gilead (consulting and payment or honoraria for lectures, presentations, speaker’s bureaus, manuscript writing, or educational events), Janssen (payment or honoraria for lectures, presentations, speaker’s bureaus, manuscript writing, or educational events), Merck (payment or honoraria for lectures, presentations, speaker’s bureaus, manuscript writing, or educational events), Theratechnologies (payment or honoraria for lectures, presentations, speaker’s bureaus, manuscript writing, or educational events), and ViiV Healthcare (consulting and payment or honoraria for lectures, presentations, speaker’s bureaus, manuscript writing, or educational events) and support for attending meetings and/or travel from Gilead and Pfizer, outside of the submitted work. C. H., C. L., R. D., K. Y. S., C. A., and W. R. S. are employees of ViiV Healthcare and stockholders of GSK. K. Y. S. also reports a role as ViiV Employee-Head of Research and Development and as a member of the ViiV Leadership Team. C. M. E., A. A., Y. W., S. L. F., and S. T. are employees and stockholders of GSK. S. L. F. also reports that GSK provides support for travel and registration to conferences as relevant and a patent application with GSK (author is named as an inventor on the patent application for a Method of Treating HIV with Cabotegravir and Rilpivirine). S. T. also reports stocks in Haleon. H. C., V. v. E., R. V. S.-R., and K. V. are employees and stockholders of Janssen, Pharmaceutical Companies of Johnson & Johnson. V. v. E. also reports the following: the US application or Patent Cooperation Treaty international application number 62/870,413 filed on 3 July 2019 (TIP1068USPSP1 Methods of Treating HIV. The disclosure is directed to the use of rilpivirine, or a salt thereof, to treat HIV infections in pediatric subjects). All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
Comment in
-
Long-Acting Cabotegravir and Rilpivirine: Innovation, New Challenges, and Opportunities.Clin Infect Dis. 2023 May 3;76(9):1655-1657. doi: 10.1093/cid/ciad024. Clin Infect Dis. 2023. PMID: 36660823 No abstract available.
References
-
- Murphy EL, Collier AC, Kalish LA, et al. . Highly active antiretroviral therapy decreases mortality and morbidity in patients with advanced HIV disease. Ann Intern Med 2001; 135:17–26. - PubMed
-
- US Department of Health and Human Services . Guidelines for the use of antiretroviral agents in adults and adolescents with HIV. Available at:https://clinicalinfo.hiv.gov/en/guidelines/hiv-clinical-guidelines-adult.... Accessed 1 September 2022.
-
- De Los Rios P, Young B, Marcotullio S, et al. . 1329. Experiences and emotional challenges of antiretroviral treatment (ART)—findings from the positive perspectives study. Open Forum Infect Dis 2019; 6(Suppl 2):S481.
