

Cost of Inpatient Falls and Cost-Benefit Analysis of Implementation of an Evidence-Based Fall Prevention Program
- PMID: 36662505
- PMCID: PMC9860521
- DOI: 10.1001/jamahealthforum.2022.5125
Cost of Inpatient Falls and Cost-Benefit Analysis of Implementation of an Evidence-Based Fall Prevention Program
Abstract
Importance: There is insufficient research on the costs of patient falls in health care systems, a leading source of nonreimbursable adverse events.
Objective: To report the costs of inpatient falls and the cost savings associated with implementation of an evidence-based fall prevention program.
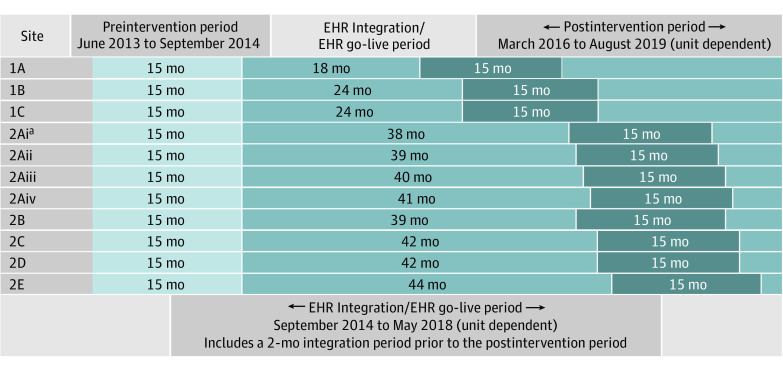
Design, setting, and participants: In this economic evaluation, a matched case-control study used the findings from an interrupted time series analysis that assessed changes in fall rates following implementation of an evidence-based fall prevention program to understand the cost of inpatient falls. An economic analysis was then performed to assess the cost benefits associated with program implementation across 2 US health care systems from June 1, 2013, to August 31, 2019, in New York, New York, and Boston, Massachusetts. All adults hospitalized in participating units were included in the analysis. Data analysis was performed from October 2021 to November 2022.
Interventions: Evidence-based fall prevention program implemented in 33 medical and surgical units in 8 hospitals.
Main outcomes and measures: Primary outcome was cost of inpatient falls. Secondary outcome was the costs and cost savings associated with the evidence-based fall prevention program.
Results: A total of 10 176 patients who had a fall event (injurious or noninjurious) with 29 161 matched controls (no fall event) were included in the case-control study and the economic analysis (51.9% were 65-74 years of age, 67.1% were White, and 53.6% were male). Before the intervention, there were 2503 falls and 900 injuries; after the intervention, there were 2078 falls and 758 injuries. Based on a 19% reduction in falls and 20% reduction in injurious falls from the beginning to the end of the postintervention period, the economic analysis demonstrated that noninjurious and injurious falls were associated with cost increases of $35 365 and $36 776, respectively. The implementation of the evidence-based fall prevention program was associated with $14 600 in net avoided costs per 1000 patient-days.
Conclusions and relevance: This economic evaluation found that fall-related adverse events represented a clinical and financial burden to health care systems and that the current Medicare policy limits reimbursement. In this study, costs of falls only differed marginally by injury level. Policies that incentivize organizations to implement evidence-based strategies that reduce the incidence of all falls may be effective in reducing both harm and costs.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
