

Neuromuscular Weakness and Paralysis Produced by Snakebite Envenoming: Mechanisms and Proposed Standards for Clinical Assessment
- PMID: 36668869
- PMCID: PMC9861841
- DOI: 10.3390/toxins15010049
Neuromuscular Weakness and Paralysis Produced by Snakebite Envenoming: Mechanisms and Proposed Standards for Clinical Assessment
Abstract
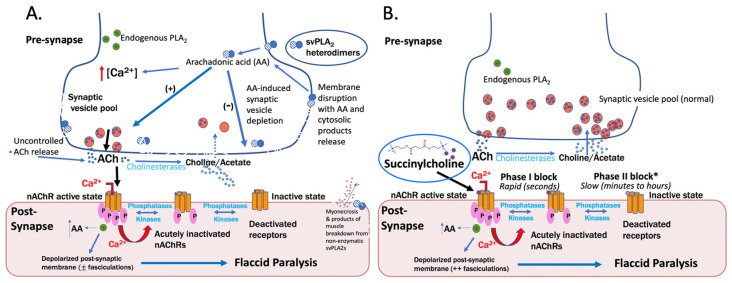
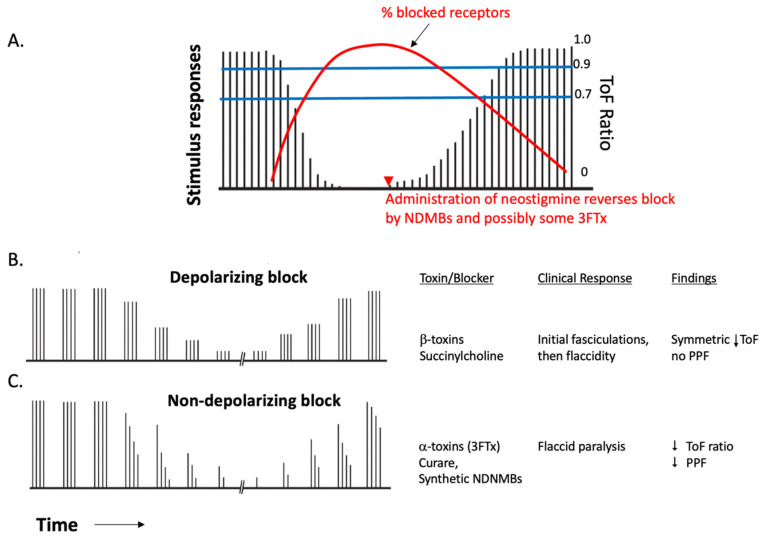
Respiratory and airway-protective muscle weakness caused by the blockade of neuromuscular transmission is a major cause of early mortality from snakebite envenoming (SBE). Once weakness is manifest, antivenom appears to be of limited effectiveness in improving neuromuscular function. Herein, we review the topic of venom-induced neuromuscular blockade and consider the utility of adopting clinical management methods originally developed for the safe use of neuromuscular blocking agents by anesthesiologists in operating rooms and critical care units. Failure to quantify neuromuscular weakness in SBE is predicted to cause the same significant morbidity that is associated with failure to do so in the context of using a clinical neuromuscular block in surgery and critical care. The quantitative monitoring of a neuromuscular block, and an understanding of its neurophysiological characteristics, enables an objective measurement of weakness that may otherwise be overlooked by traditional clinical examination at the bedside. This is important for the initial assessment and the monitoring of recovery from neurotoxic envenoming. Adopting these methods will also be critical to the conduct of future clinical trials of toxin-inhibiting drugs and antivenoms being tested for the reversal of venom-induced neuromuscular block.
Keywords: ToF; anesthesia; neuromuscular junction; neurotoxin; paralysis; postsynaptic; presynaptic; snakebite; train-of-four; weakness.
Conflict of interest statement
P.E.B. and M.R.L. own stock in Ophirex, Inc., a company developing novel snakebite treatments. M.A. and A.B. have no conflict of interest to declare.
Figures
References
-
- Williams D.J., Faiz M.A., Abela-Ridder B., Ainsworth S., Bulfone T.C., Nickerson A.D., Habib A.G., Junghanss T., Fan H.W., Turner M., et al. Strategy for a Globally Coordinated Response to a Priority Neglected Tropical Disease: Snakebite Envenoming. PLoS Negl. Trop. Dis. 2019;13:e0007059. doi: 10.1371/journal.pntd.0007059. - DOI - PMC - PubMed
-
- Hung H.T., Höjer J., Du N.T. Clinical Features of 60 Consecutive ICU-Treated Patients Envenomed by Bungarus Multicinctus. Southeast Asian J. Trop. Med. Public Health. 2009;40:518–524. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
