

Multicentre positive deviance to reduce adverse events and length of stay after pulmonary resection
- PMID: 36669834
- PMCID: PMC9872471
- DOI: 10.1136/bmjoq-2022-001997
Multicentre positive deviance to reduce adverse events and length of stay after pulmonary resection
Abstract
Background: Postoperative adverse events (AEs) following pulmonary resection enormously impact patient well-being, length of stay (LOS) and healthcare costs. Standardised AE data collection can be used to identify positive outliers demonstrating positive deviance (PD) who may be helpful to inform the best practice. Here, we describe our initial experience of a novel quality improvement process using PD to reduce LOS and AEs.
Methods: AE rates and LOS were collected from four centres (2014-2020) using a common dictionary. Surgeons repeatedly participated in 60 to 90 min seminars consisting of the following process: identify outcome and procedure targeted, review relevant best evidence literature, view all data anonymised by surgeon or centre (if multicentre), choose and reveal identity of best performance PD outliers, who discuss their management principles while all receive self-evaluation reports, followed by collegial discussion to generate consensus recommendations, voted by all. We assessed overall impact on AEs and LOS using aggregate data in a before/after analysis.
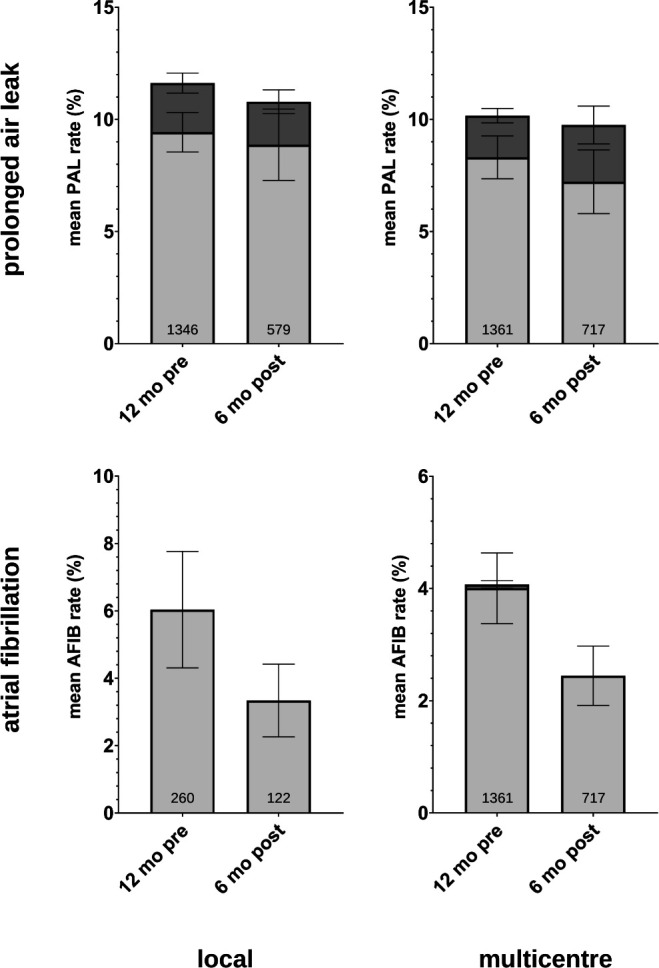
Results: A total of 131 surgeons (average 12/seminar) participated in 11 PD seminars (8 local and 3 multicentre), yielding 85 consensus recommendation (average 8/seminar). Median LOS following lobectomy decreased from 4.0 to 3.0 days (p=0.04) following local PD seminars and from 4.0 to 3.5 days (p=0.11) following multicentre seminars. Trends for reductions in multiple AE rates were also observed.
Conclusion: While limited by the longitudinal design, these findings provide preliminary support for this data-driven, collegial and actionable quality improvement process to help standardise and improve patient care, and merits further more rigorous investigation.
Keywords: Adverse events, epidemiology and detection; Continuous quality improvement; Postoperative Care; Quality improvement methodologies; Surgery.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources