

Population-Based Screening Using Low-Dose Chest Computed Tomography: A Systematic Review of Health Economic Evaluations
- PMID: 36670332
- PMCID: PMC10020316
- DOI: 10.1007/s40273-022-01238-3
Population-Based Screening Using Low-Dose Chest Computed Tomography: A Systematic Review of Health Economic Evaluations
Abstract
Background: Chest low-dose computed tomography (LDCT) is a promising technology for population-based screening because it is non-invasive, relatively inexpensive, associated with low radiation and highly sensitive to lung cancer. To improve the cost-effectiveness of lung cancer screening, simultaneous screening for other diseases could be considered. This systematic review was conducted to analyse studies that published evidence on the cost-effectiveness of chest LDCT screening programs for different diseases.
Methods: Scopus and PubMed were searched for English publications (1 January 2011-22 July 2022) using search terms related to screening, computed tomography and cost-effectiveness. An additional search specifically searched for the cost-effectiveness of screening for lung cancer, chronic obstructive pulmonary disease or cardiovascular disease. Included publications should present a full health economic evaluation of population screening with chest LDCT. The extracted data included the disease screened for, model type, country context of screening, inclusion of comorbidities or incidental findings, incremental costs, incremental effects and the resulting cost-effectiveness ratio amongst others. Reporting quality was assessed using the 2022 Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist.
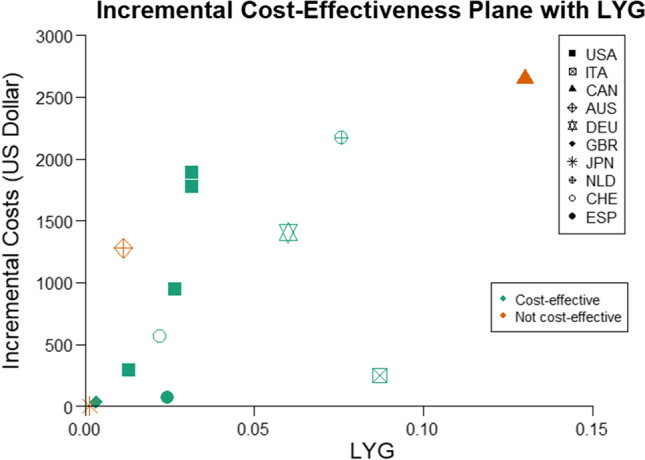
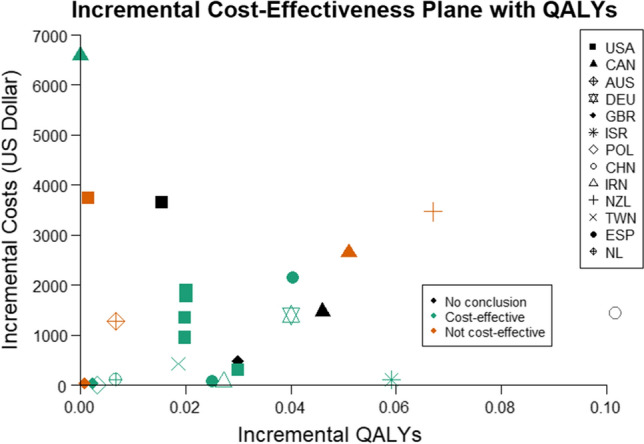
Results: The search yielded 1799 unique papers, of which 43 were included. Most papers focused on lung cancer screening (n = 40), and three were on coronary calcium scoring. Microsimulation was the most commonly applied modelling type (n = 16), followed by life table analysis (n = 10) and Markov cohort models (n = 10). Studies reflected the healthcare context of the US (n = 15), Canada (n = 4), the UK (n = 3) and 13 other countries. The reported incremental cost-effectiveness ratio ranged from US$10,000 to US$90,000/quality-adjusted life year (QALY) for lung cancer screening compared to no screening and was US$15,900/QALY-US$45,300/QALY for coronary calcium scoring compared to no screening.
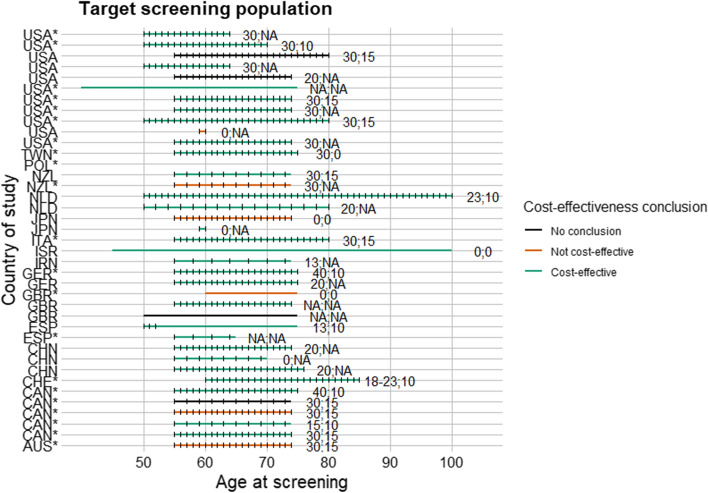
Discussion: Almost all health economic evaluations of LDCT screening focused on lung cancer. Literature regarding the health economic benefits of simultaneous LDCT screening for multiple diseases is absent. Most studies suggest LDCT screening is cost-effective for current and former smokers aged 55-74 with a minimum of 30 pack-years of smoking history. Consequently, more evidence on LDCT is needed to support further cost-effectiveness analyses. Preferably evidence on simultaneous screening for multiple diseases is needed, but alternatively, on single-disease screening.
Registration of systematic review: Prospective Register of Ongoing Systematic Reviews registration CRD42021290228 can be accessed https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=290228 .
© 2023. The Author(s).
Conflict of interest statement
R. Vliegenthart is supported by an institutional research grant from Siemens Healthineers and reports speaker’s fees from Siemens Healthineers and Bayer. In addition, M.J. IJzerman has held advisory board roles with respect to Illumina, and his institution (University of Melbourne) receives unrestricted research funding from Illumina. H. Koffijberg, C.M. Behr and M.J. Oude Wolcherink declare that they have no conflict of interest.
Figures
Similar articles
-
Systematic review of the cost-effectiveness of screening for lung cancer with low dose computed tomography.Lung Cancer. 2022 Aug;170:20-33. doi: 10.1016/j.lungcan.2022.05.005. Epub 2022 May 13. Lung Cancer. 2022. PMID: 35700629
-
Cost-effectiveness of Low-Dose Computed Tomography With a Plasma-Based Biomarker for Lung Cancer Screening in China.JAMA Netw Open. 2022 May 2;5(5):e2213634. doi: 10.1001/jamanetworkopen.2022.13634. JAMA Netw Open. 2022. PMID: 35608858 Free PMC article.
-
Economic evaluation of low-dose computed tomography for lung cancer screening among high-risk individuals - evidence from Hungary based on the HUNCHEST-II study.BMC Health Serv Res. 2024 Dec 3;24(1):1537. doi: 10.1186/s12913-024-11828-w. BMC Health Serv Res. 2024. PMID: 39627793 Free PMC article.
-
Cost-effectiveness and health impact of lung cancer screening with low-dose computed tomography for never smokers in Japan and the United States: a modelling study.BMC Pulm Med. 2022 Jan 8;22(1):19. doi: 10.1186/s12890-021-01805-y. BMC Pulm Med. 2022. PMID: 34996423 Free PMC article.
-
[Cost-effectiveness of lung cancer screening worldwide: a systematic review].Zhonghua Liu Xing Bing Xue Za Zhi. 2019 Feb 10;40(2):218-226. doi: 10.3760/cma.j.issn.0254-6450.2019.02.018. Zhonghua Liu Xing Bing Xue Za Zhi. 2019. PMID: 30744276 Chinese.
Cited by
-
New Perspectives on Lung Cancer Screening and Artificial Intelligence.Life (Basel). 2025 Mar 19;15(3):498. doi: 10.3390/life15030498. Life (Basel). 2025. PMID: 40141842 Free PMC article. Review.
-
Model-Based Cost-Utility Analysis of Combined Low-Dose Computed Tomography Screening for Lung Cancer, Chronic Obstructive Pulmonary Disease, and Cardiovascular Disease.JTO Clin Res Rep. 2025 Feb 19;6(5):100813. doi: 10.1016/j.jtocrr.2025.100813. eCollection 2025 May. JTO Clin Res Rep. 2025. PMID: 40236262 Free PMC article.
-
Advances in early detection of non-small cell lung cancer: A comprehensive review.Cancer Med. 2024 Sep;13(18):e70156. doi: 10.1002/cam4.70156. Cancer Med. 2024. PMID: 39300939 Free PMC article. Review.
-
A Systematic Literature Review of Modelling Approaches to Evaluate the Cost Effectiveness of PET/CT for Therapy Response Monitoring in Oncology.Pharmacoeconomics. 2025 Feb;43(2):133-151. doi: 10.1007/s40273-024-01447-y. Epub 2024 Nov 3. Pharmacoeconomics. 2025. PMID: 39488797 Free PMC article.
References
-
- WHO Screening programmes: a short guide. WHO Press. 2020;1:1–70.
-
- Drummond MF, Sculpher MJ, Claxton K, et al. Methods for the economic evaluation of health care programmes. 3. Oxford: Oxford University Press; 2015.
-
- United States Preventitive Services Task Force (2021) U.S. Preventive Services Task Force Issues Draft Recommendation Statement on Screening for Lung Cancer. Washington, D.C.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
